Dansket
Content Type
Store
Profiles
Forums
Blogs
Events
Frequently Asked Questions
Gallery
Downloads
Glossary
Links Directory
Questions
Jobs
Vendors
Everything posted by Dansket
-
When the Transfusion Services becomes aware of such a situation, you have no choice but to demand unit be returned and discard it.
-
We are controlled, to a greater or lesser extent, by regulators as to what we can/cannot do. Talking with donor center personnel over the years, they have no 'wiggle-room' when it comes to compliance with FDA regulations. Transfusion Services inspections that are conducted by FDA surrogates are not nearly as stringent. Transfusion Services have the option to select a regulator (AABB, CAP, JCAHO, HFAP), Donor Centers have no choice.
-
The FDA's decision may have to do more with the level of control. Donor Centers are inspected directly by the FDA, whereas surrogates (AABB, CAP, etc.) inspect hospital transfusion services. As John C. Staley stated "This started being a hot topic 10-15 years ago." While Transfusion Services continue to challenge the FDA interpretations, Donor Centers don't!
-
Our SOP requires that newborns, who test negative with anti-D by immediate-spin test, must be tested for Weak D using anti-D antiserum formulated for Weak D testing. If the Weak D Control is agglutinated, we report Rh type of the newborn as "Indeterminate" and "RhIG indicated" for the mother if the mother is Rh negative.
-

At my hospital we manually enter Type and Screen results....
Dansket replied to paddleking's topic in Transfusion Services
Does user enter interpretations manually or does the computer generate interpretations automatically? -
At my hospital we manually enter Type and Screen results....
Dansket replied to paddleking's topic in Transfusion Services
When user enters Type and Screen results into computer, are intermediate results entered (anti-A, anti-B, etc) or only the interpretations, e.g. APOS, BNEG etc.? Are results of Antibody screen for Cell1 and Cell2 entered or just interpretation, e.g. Positive or Negative? -
We print an individual Results report for each specimen which is identified by a barcoded sample ID label affixed by the operator. The operator then scans the sample ID from the Results report into Meditech enters and files the results. The printed report is then filed in the Supervisor's Review basket. As Supervisor, I repeat the process for each individual report and verify results on report match results entered in Meditech. I sign and date the report and file the report in a binder. This binder is made available for inspectors to indicate this Quality Review process.
-
An order for a second venipuncture is automatically reflexed by Meditech based on testing done on the initial blood sample collected for Type and Screen. Our phlebotomists have no role in determining whether or not a second blood sample is required. If there is no ABO on file and testing of the initial blood sample with anti-A,B yields a positive test result (patient is not group O), Meditech automatically creates a new order for an ABO verification test that requires collection of a second blood sample. This results in printing of specimen collection labels on the Phlebotomy Label Printer. Transfusion Services does not accept unsolicited blood samples collected for the ABO verification testing.
-
Testing the same blood sample twice will not detect WBIT. That is why we draw a second blood sample from a different venipuncture from patients who initially type not group O. We are not AABB accredited.
-
Electronic crossmatch with Meditech
Dansket replied to BloodbankZ's topic in Computer Systems / Software / ISBT128
To prevent Meditech from qualifying a patient for EXM when mixed-field agglutination is detected, then detection of a mixed-field result must be entered into Meditech in some manner. In this way, Meditech can react to that test result using rules, reflexing tests, calculations and interpretations. Currently, if mixed-field agglutination is detected in the Anti-A, Anti-B, Anti-A,B and/or Anti-D test, how is that mixed-field test result entered into Meditech? What is your current policy for documenting selection of blood for transfusion in Meditech when mixed-field agglutination is detected in ABO/Rh grouping tests? For example, do you automatically select group O when mixed-field is detected in ABO grouping? Rh negative when mixed-field is detected in Rh grouping? How is your Crossmatch test configured? Do you use a Meditech Blood Issue routine in real-time when releasing blood to Nursing, et al? -
I have run an R1R1 cell for a positive control and an rr cell for negative control for Weak D testing in Gel since 1996 without any complaints from numerous inspectors, CAP and AABB.
-
If the current antibody screen is negative we issue electronically crossmatched units untested for Lea. If the current antibody screen is positive, we issue IgG-crossmatch compatible units untested for Lea
-
I believe there is a field for Visual Inspection on page 1 of the product dictionary. If you enter Y, users are prompted during product login.
-
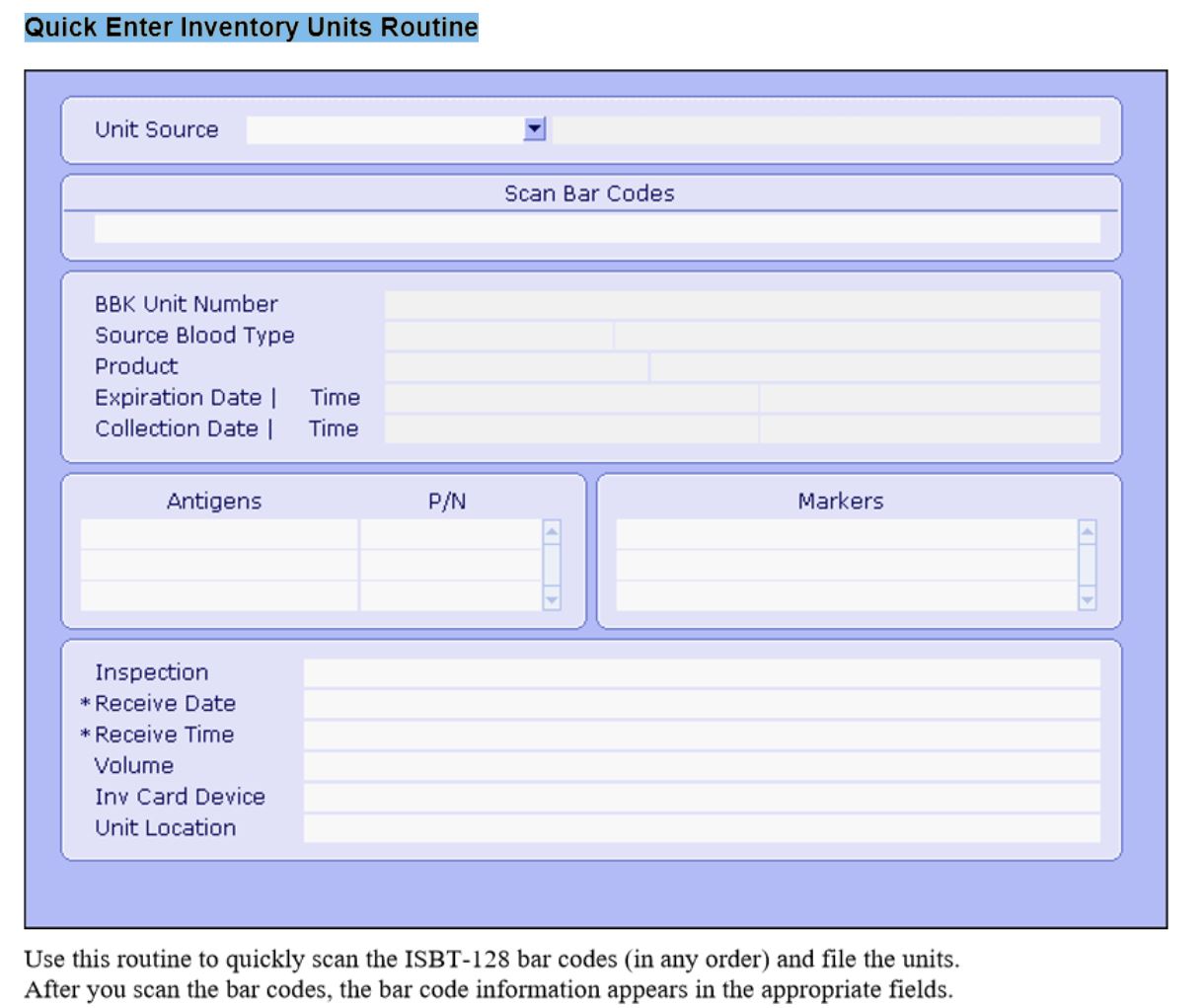
Entering Inventory Meditech 6.16
Dansket replied to richj's topic in Computer Systems / Software / ISBT128
Use the Quick Enter Units Inventory routine.
-
What temperature of the ice packs do you consider unaccepatable? What temperature of the unit do you consider unacceptable? In the United States, holding Thawed FFP in a cooler is considered storage by the FDA. So whatever is the acceptable storage temperature of Thawed FFP would apply.
-
Let me spin this differently. I'm unlikely to detect an anti-A1 or any other weakly reactive (1-2+) IgM antibody in routine room-temperature gel testing. Secondly, I have eliminated the immediate-spin crossmatch in favor of an electronic crossmatch to detect ABO incompatibility between donor and recipient. Lastly, by adopting the electronic crossmatch, I have accepted that any reactivity (limited to room-temperature) between donor and recipient (not demonstrated to be due to anti-A and/or anti-B) is rendered clinically irrelevant!
-
In Meditech, user can designate whether an antibody is/is not clinically significant and can also designate corresponding antigen-negatives. In the case of anti-A1, you could create two 'anti-A1' entries in the 'antibody file'. One would be designated "clinically-significant' and that A2 cells were 'antigen-negative'. The second entry in the antibody file would not be designated 'clinically-significant' and the 'antigen-negative' field left blank. For patients with an anti-A1 that reacts as 37C, computer would require A2 red cells for crossmatch. Patients with anti-A1 that does not react at 37C would not require A2 cells.
-
Specimen Processing Flow Chart View File This flow chart was originally created for training travelers, but now is used for new hires as well. A significant departure from the typical transfusion service is steps taken on certain blood samples prior to centrifugation. The TYPENEX code is entered from the blood sample container to verify that it was correctly entered into Meditech by the phlebotomist. It is better to detect problems prior to testing than when attempting to release blood component to Nursing. Submitter Dansket Submitted 04/20/2017 Category Educational Materials
-

Version 1.0.0
65 downloads
This flow chart was originally created for training travelers, but now is used for new hires as well. A significant departure from the typical transfusion service is steps taken on certain blood samples prior to centrifugation. The TYPENEX code is entered from the blood sample container to verify that it was correctly entered into Meditech by the phlebotomist. It is better to detect problems prior to testing than when attempting to release blood component to Nursing. -
TYPENEX flow chart View File I use this flow chart for training new hires in Transfusion Services. This gives them a graphical overview, of not only how the TYPENEX code is tracked from specimen collection to blood infusion, but also the workflow in our section. Submitter Dansket Submitted 04/18/2017 Category Educational Materials
-

Version 1.0.0
55 downloads
I use this flow chart for training new hires in Transfusion Services. This gives them a graphical overview, of not only how the TYPENEX code is tracked from specimen collection to blood infusion, but also the workflow in our section. -
Labeling Blood Components with Compatibility Info
Dansket replied to VirginiaBG's topic in Transfusion Services
See my download in the library "Blood Issue Cause and Effect". The process starts with a tagged (form attached immediately after crossmatch) blood component removed from storage. -
Do you have data, percentage of positive blood cultures of donor units implicated in a febrile reaction to blood transfusion?
-
An autocontrol is an indirect antiglobulin test that includes both patient serum/plasma and patient rbc incubated together at 37C and subsequently tested with antihuman globulin reagent. Methodology includes the standard tube test, Gel test, PEG test etc.
-
I don't trust Nursing. They may have put the unit into storage on the Nursing station or mishandled the unit in attempts to warm it up or cool it down. I draw the line at 30 minutes, no exceptions. I don't get into "what if 31 minutes?, what if 32 minutes?, what if 33 minutes"? According to your process, would you reissue blood returned unused and within temperature regardless of time out of storage? Are there no exceptions for time out of storage?