-
 We use Ranger blood warmers in OR and sometimes other locations (but Belmonts for rapid infusion). I have been presented a question asking if we can still use them for blood because they warm the blood to 41C, but UpToDate says that blood shouldn't be warmed above 40C. I see no references listed in UPToDate to support their 40C requirement. We test the alarms on Ranger blood warmers, and they must alarm by 43C. From the Ranger Service manual: "The Ranger blood/fluid warming system is designed to warm blood, blood products, and liquids and deliver these at flow rates from KVO to 500 mL/min. At these flow rates, the device maintains fluid output temperatures ranging from 33°C to 41°C (Note: This is for room temperature fluids only). It takes less than two minutes to warm up to the 41°C ±1 set point temperature. The alert points on the Model 245 are 43°C ±1 and 46°C [+3, -2°C]." The 2002 AABB Guidelines for the Use of Blood Warming Devices says "The effectiveness of a blood warmer is limited by the flow rate of the infusion and the heating technology of the device in use. Most do not delivery normothermic (37C) fluids at very rapid flow rates--most reach a temperature of only 33 C to 36 C." These devices are FDA approved for blood transfusion, right? Can anyone supply an answer to the question of why (or why not) they are okay to use according to manufacturer's instructions, but UpToDate says not to warm blood above 40C?
We use Ranger blood warmers in OR and sometimes other locations (but Belmonts for rapid infusion). I have been presented a question asking if we can still use them for blood because they warm the blood to 41C, but UpToDate says that blood shouldn't be warmed above 40C. I see no references listed in UPToDate to support their 40C requirement. We test the alarms on Ranger blood warmers, and they must alarm by 43C. From the Ranger Service manual: "The Ranger blood/fluid warming system is designed to warm blood, blood products, and liquids and deliver these at flow rates from KVO to 500 mL/min. At these flow rates, the device maintains fluid output temperatures ranging from 33°C to 41°C (Note: This is for room temperature fluids only). It takes less than two minutes to warm up to the 41°C ±1 set point temperature. The alert points on the Model 245 are 43°C ±1 and 46°C [+3, -2°C]." The 2002 AABB Guidelines for the Use of Blood Warming Devices says "The effectiveness of a blood warmer is limited by the flow rate of the infusion and the heating technology of the device in use. Most do not delivery normothermic (37C) fluids at very rapid flow rates--most reach a temperature of only 33 C to 36 C." These devices are FDA approved for blood transfusion, right? Can anyone supply an answer to the question of why (or why not) they are okay to use according to manufacturer's instructions, but UpToDate says not to warm blood above 40C? -
-
Almost all our platelets are pathogen reduced so they aren't much more of a worry than usual in an MTP. Does anyone know how likely TA-GVHD is in patients on drugs like fludarabine and cladribine? The inserts just say that the patients should get irradiated units, but I would guess that the risk is lower than someone 4 months post stem cell transplant. I've heard that TA-GVHD is 95% fatal, but I think that is in a recent transplant cohort. Bleeding to death is also fatal. The nuance is in the ED doc's perception of how likely it is that the patient is bleeding to death. Most of our irradiation patients are only candidates for transplant so I think their risk is small if they don't get irradiated blood in an emergency. They can probably postpone the transplant. In our most recent case at one of our small hospitals, I could see that the patient had no recent transplant and was not on those purine analog drugs so felt his risk was low and he did fine after getting 1 irradiated RBC and one non then going to IR to fix his second spontaneous splenic rupture in the setting of lymphoma and DOAC.
-
-
If a small site that doesn't stock irradiated blood has to give emergency transfusion or a bigger place can't provide several rounds of an MTP that are irradiated, what are the risks? I know that patients who had a Stem Cell transplant in recent years must get irradiated products or face a very dangerous form of GVHD. I know that patients on purine analog drugs should get irradiated blood, but I don't know how dangerous it is if they don't. Otherwise, most patients seem to get irradiated because they are candidates for future transplants. Clearly, we can't let patients bleed to death but, if we get an MTP order on someone our system says needs irradiated blood, what do we tell the pathologist or ED doc about the risk? Our patient was a non-Hodgkins lymphoma who has not had a transplant, and I see no evidence of cladribine or fludarabine drugs in his list, so I think he is okay. I know that the doctors are the ones taking responsibility, but I want to understand the relative risks of various patient conditions with regard to GVHD.
-
Some of the worst hemolysis I have seen was in clostridium septicemia. Both cases were fatal.
-
 Ensis01 reacted to a post in a topic:
FDA requirements for 2 people to issue blood products for transfusion.
Ensis01 reacted to a post in a topic:
FDA requirements for 2 people to issue blood products for transfusion.
-
Do you do anything to make them actually "blind", or do you trust your staff not to look up the original results?
-
-
Can we purchase this in the US yet? What company is making it?
-
-
Mabel Adams reacted to a post in a topic:
Source of advice on transfusing patients with mismatched stem cell/bone marrow transplants?
-
-
Does anyone allow electronic crossmatch to be used in cases where a prior marrow transplant will never result in the usual reverse type on the patient (for example B to A)? We have a discrepancy blood type test in our computer that doesn't require the usual truth tables be met that we currently use for these patients. We require 2 separate specimens to be typed before we give any RBCs that aren't group O. We require 2 individuals to review any results turned out using the discrepancy test (this doesn't mean mistakes couldn't happen). We could have a patient with a cold agglutinin that would make an IS crossmatch incompatible (although maybe immunosuppressed patients won't make those?). I just want to see if anyone else has worked through all the logic involved in making sure patients are safely transfused yet the testing is appropriate to the need.
-
Mabel Adams reacted to a post in a topic:
Source of advice on transfusing patients with mismatched stem cell/bone marrow transplants?
-
If you issue blood via a pneumatic tube system, this introduces some additional processes.
-
We sometimes find them negative in PEG. If that or a DTT treated screen is negative, we give units as electronic crossmatched (K matched if DTT used). Anti-CD38 is not a clinically significant antibody, and we have a negative DTT screen we can turn out which makes the computer happy.
-
-
We have patients that come home from university hospitals after transplants that we need to transfuse. We can often find in their charts the recommendations of the transplant center on what donor types to use. When we can't, I would like to have a definitive source on what blood type we should transfuse to these patients. The current patient was B pos, now A pos after a transplant 6 years ago. His chart says they consider him "cured". He forward types as A and back types as AB, as expected. I think we should be giving him A pos RBCs but I want a definitive source to cite in his notes.
-
Mabel Adams reacted to a post in a topic:
Patient with anti-D, anti-C is negative with other reagent cells but incompatible with most units.
-
Mabel Adams reacted to a post in a topic:
Patient with anti-D, anti-C is negative with other reagent cells but incompatible with most units.
-
Yanxia reacted to a post in a topic:
Patient with anti-D, anti-C is negative with other reagent cells but incompatible with most units.
-
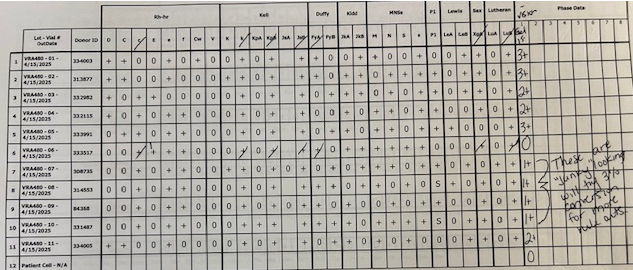
I expected to see a stronger reaction with the P1 cells labeled as "strong", but it does react with only the P1+ cells. Maybe P1 persists better on donor cells than reagent cells.
-
Mabel Adams reacted to a post in a topic:
Patient with anti-D, anti-C is negative with other reagent cells but incompatible with most units.
-
Mabel Adams reacted to a post in a topic:
Patient with anti-D, anti-C is negative with other reagent cells but incompatible with most units.
-
Yanxia reacted to a post in a topic:
Patient with anti-D, anti-C is negative with other reagent cells but incompatible with most units.
-
We need to determine how we will issue cold stored platelets in a massive transfusion. We would like to put them in coolers packed like RBCs, but we found that they get too cold. Has anyone identified a packing method that works well for CSP but doesn't mean we have to annually check 16 coolers by two different packing methods so we can use them for either CSP or RBCs? We may have to dedicate some coolers to platelets but would rather not.
-
The H explanation seems plausible although we didn't see much difference between A and O donors in terms of reaction strengths. I attached the original panel using Ortho 0.8% pre-diluted cells. Maybe these keep their H antigen better than the 3% cells we converted to 0.8%. The panel shown was only a few days from expiring. The 3% cells expire May 9th. This seems backwards from what we would expect if the antigens were weakening in storage. However, they are from different manufacturers and in different diluents. The 3% cells were from Immucor.
-
Yanxia reacted to a post in a topic:
Patient with anti-D, anti-C is negative with other reagent cells but incompatible with most units.
-
That's a good question. The new sample was tested against Ortho 0.8% screen cells which were both positive due to her anti-D/C/G. Four C & D neg 3% panel cells were converted to 0.8% and run in gel with a 30-minute incubation. They were all negative. Then the new specimen was also used to crossmatch about 10 units, and we found 3 were compatible. I checked to see if she was getting TPN but don't see any. Sometimes that fats and proteins in the nutrition IV cause strange reactions. Usually, I have seen a positive DAT with it. If you can further describe the sort of protein you are thinking of, I would appreciate it.
-
Yanxia reacted to a post in a topic:
Patient with anti-D, anti-C is negative with other reagent cells but incompatible with most units.
-
I noticed that pattern that suggests anti-G also. In transfusion, it doesn't matter whether it is anti-D/C or anti-G or a combination of them, right? We would pursue it in pregnant patients. Could she have been exposed to G without being exposed to either D or C? I feel like I've read that this is extremely rare, but not impossible. Yes, we find antibody to the diluent in Ortho's pre-diluted 0.8% reagent cells quite often. I believe that is what we found in the original testing besides the anti-D/C/G. When we make 0.8% suspensions from 3% cells, we use diluent 2 which lacks most of the antibiotics that are in the pre-diluted cells. It is a bit strange that the diluent antibody did not react with one cell. I have seen before where the antibody seems to have a predilection for some Rh antigens, and it seems like the antibiotic almost complexes with them on the RBC surface (maybe sterically). I think an antibody to the gel diluent explains why the panel went to negative except for with the D or C positive cells, Unfortunately, the reaction difference causing my consternation is between 3% reagent cells and donor cells suspended in the same diluent. If there were antibodies to the diluent that the 3% reagent cells were originally suspended in, I would expect those cells to react in gel rather than the donor units. I wonder if there is something in AS-1 that coats the RBCs to which this patient has an antibody. The negative reactions would then be due to lower levels in some donors compared to those eliciting stronger reactions. I had was told years ago that 3% cells freshly converted to 0.8% were somewhat more sensitive in Ortho gel testing, but this is acting in reverse. Also, I have heard that units are preserved to maximize their function after transfusion, not to stabilize antigens, whereas reagent cells are preserved to maximize antigen expression. Again, this is behaving backwards. I wonder if we should have done more antibody testing in PEG. Some specificities "like" PEG better than gel. Maybe we would have identified a 3rd antibody. It will be interesting to see if, in future testing, she makes another alloantibody. Appreciate this and any other input.
