SbbPerson
Content Type
Store
Profiles
Forums
Blogs
Events
Frequently Asked Questions
Gallery
Downloads
Glossary
Links Directory
Questions
Jobs
Vendors
Everything posted by SbbPerson
-
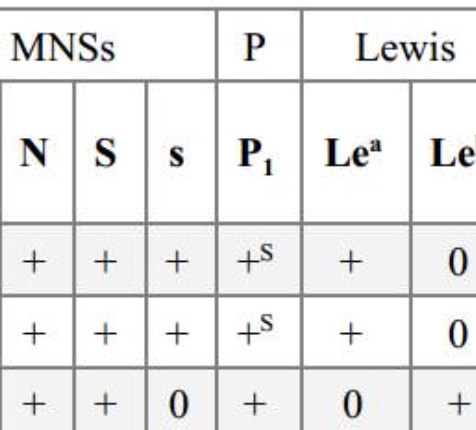
What is ‘+s’? Please look at attached antigram. It’s in the reaction column of the P1 antibody. Anybody knows? Thank you

-
 "Sure it could happen ,,, and here's how... one of the parents perhaps has the Bombay phenotype"
"Sure it could happen ,,, and here's how... one of the parents perhaps has the Bombay phenotype" -
I disagree. Most gel cards and Anti-D reagents won't detect DVI for patients. Fortunately I can find numerous suitable quotes, because it's true. https://labs-inc.org/pdf/361_3.pdf
-
Yes, I know. I was talking about patients on my original post.
-
"Modern anti-D reagents, while they are very good at detecting weaker forms of the D antigen, are specifically designed to NOT detect the most common form of partial D in Caucasians (DVI, or “D six”), so most Caucasian partial D patients will test as D-negative." -BloodBank Guy https://www.bbguy.org/education/glossary/glp04/
-
I think most modern Anti-D reagents won't detect DVI and these patients will test as D-negative. This is probably the answer. Anyways, this is the answer he gave his students. To me, the answer looks as vague as the question. Not "straight forward" at all. IMG_2756.heic
-
Yes, I don't think the original question setter meant the question to be a difficult one to answer. He is teaching a beginner level MLT course. He said there was only one correct "straight forward" answer. Just my opinion , but I think this person has no business teaching college level blood banking. As far as I know, he is a MLT with no experience with the tube, slide, or microplate testing methods, so I highly doubt he was talking about Anti-D reagents being the source of the discrepancy. But I could be wrong. I apologize for wasting people's time with this. I just can't understand how is he teaching medical lab science and blood banking at a local college, and handing out assignments with these sort of questions.
-
No DAT. There are no other details to the question. I’m just trying to get people’s opinion on the question. Thank you
-
"A donor unit obtained from a central blood bank was labeled as Group O, D-negative. When the hospital transfusion service confirmed the donor's type, the result was group O, D-positive. Investigation of the label issued at the blood bank verified the unit's correct labeling. How can you explain the discrepancy in the D type of this donor unit?" The person who wrote this question said it is a "critical thinking" question and there is only one correct answer.
-
I think this question is suited more for sysmex IT tech support. I don't know about these days with modern day techs, but in my experience, it's the techs that perform the cell counts using a miller disc for the KB method. If your facility uses 300 uL dose RhIg, you can use this simple equation: (%fetal cells x 50) / 30 = number of vials of RhIg required. Remember to use the "fudge factor". Example: 1.3% fetal cells calculated on Kleihauer Betke stain 1.3 X 50 = 65 ml of fetal blood 65 ml/30 = 2.2 vials of RhIG required When the number to the right of the decimal point is less than 5, round down and add one dose. Example: If the calculation comes to 2.2, give 3 vials. When the number to the right of the decimal point is greater than 5, round up and add one dose. Example: If the calculation gives 2.8, give 4 vials. source: https://hsc.ghs.org/obgyn-clinical-practice-guidelines/inpatient-obstetrics/kleihauer-betke-assay-interpretation/
-
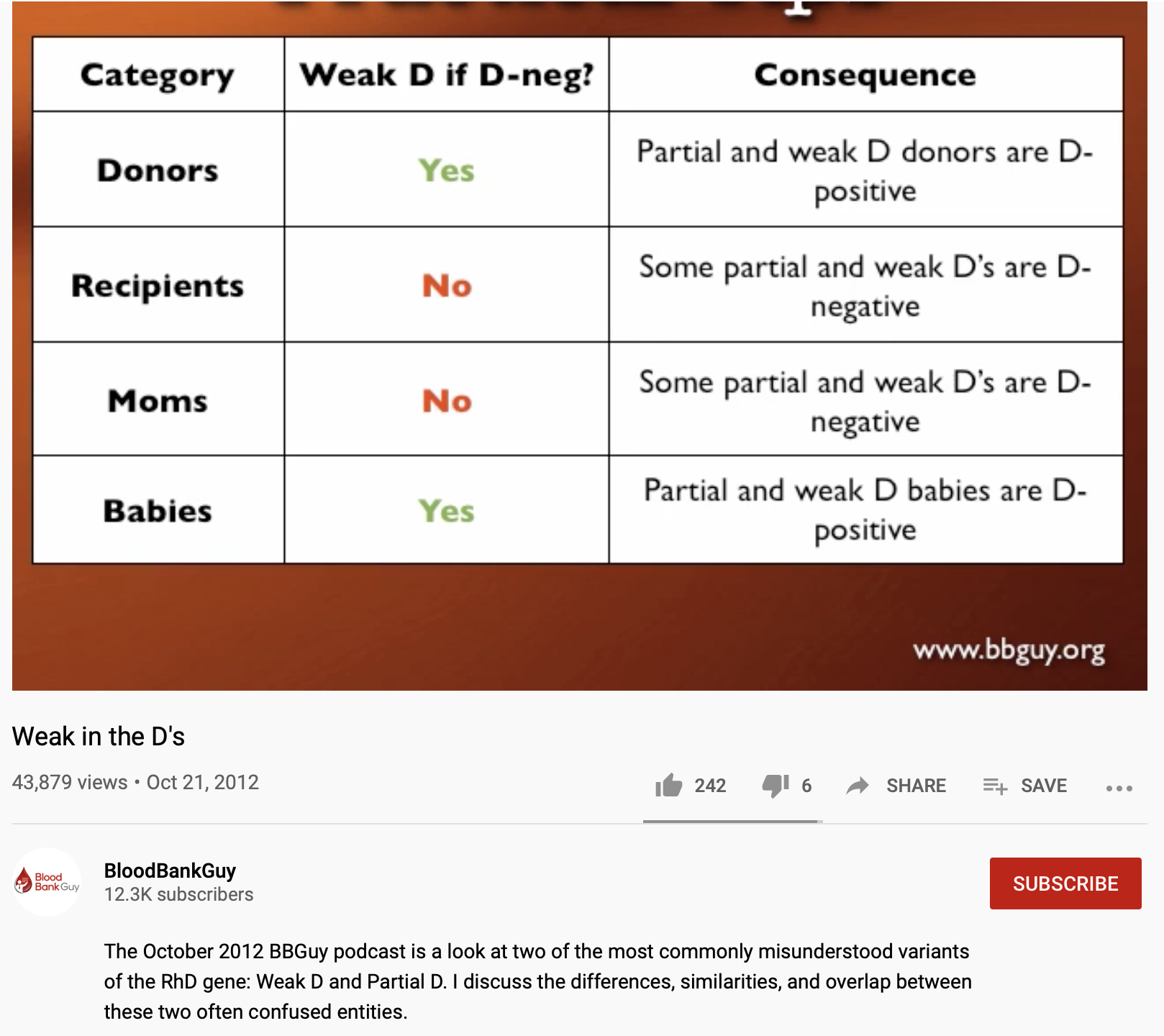
I have never heard of your references. The main texts for my course includes AABB technical manual by Fung, Harmening's Modern blood banking and transfusion services, and AABB's Standards for blood banking. I am only a part time SBB student, I work full time as a Medical Technologist. This is my final semester. You don't need to show me references I never heard of, I am certain you are right. Mom's with PARTIAL D (NOT WEAK D, WE DON'T TEST WEAK D FOR MOMS) can be typed as Rh positive, but still may form Anti-D when exposed to Rh positive red cells from baby(Modern Blood banking and transfusion services, Harmening, 7th Ed. p. 160).
-
We do not do Weak D testing on mothers here where I work. This is a common practice in America
-
We don't do Weak D testing on adults, unless if they are donating blood.
-
I never said mother with weak D. Come on Malcolm, you know I didn't say mothers with weak D.
-
You know why Malcolm. If mom is Rh negative and baby is Rh positive, mom has 16% chance of developing anti-D after her first pregnancy. Moms with partial D can be classified as Rh Positive, but may still require RhIg to prevent HDFN. Our policy is to do weak D testing on all newborns who test D negative when we do the ABO/Rh forward typing.
-
We do weak D testing on all cords bloods that test negative with Anti-D. Regardless if the mom is Rh positive or negative.
-
I am looking for an animation program or drawing program that can help me make my blood bank presentation more entertaining. Anyone knows of such program? This is my last semester in my SBB program and I am required to do a presentation. My topic is on the blocked D phenomenon and it's role in HDFN. I would love to do something like what Dr. Chaffin does for his presentations on his website www.bbguy.org . Any tips or info is greatly appreciated. Thank you.
-
Yes, you are completely right Malcolm and others. My experience is limited to common positive DAT results for OB patients, which is the ABO mismatch. Those positives are usually 1+ or weaker. That's why we always do a microscopic if we get a macroscopic negative. I forgot that Rh mismatch DATs can go from 2+ to 4+ positive, because I hardly ever come across those. Thank you.
- 28 replies
-
- 1
-

-
- direct antiglobulin test
- dat
- (and 5 more)
-
sorry, I shouldn't have said "never" ... What I really meant to say was, I always do a microscopic exam for agglutination if the immediate spin appears negative. Other people probably see a lot of macroscopically positive DATs. I don't come across too many of those. Thank you sir
- 28 replies
-
- 1
-

-
- direct antiglobulin test
- dat
- (and 5 more)
-
I think you need to do microscopic on all DATs , because IgG is only a monomer antibody and won't cause agglutination visible to the naked eye.
-
Positive antibody screen/ negative panel
SbbPerson replied to amym1586's topic in Education / Quality
I am sorry, but what does putting up "12 different antibody screens(12 different patients)" have to do with my original question? Sorry, I don't understand what you are trying to explain. My English is very poor. Can you explain with simple English or use scientific terms instead? But thank you so much for your time and knowledge . -
Where is it? I can't find it
-
Positive antibody screen/ negative panel
SbbPerson replied to amym1586's topic in Education / Quality
Thank you so much for your reply. I keep asking you questions, so sorry. But did you say 12 screen cells? Usually, we use only 2 or 3 screen cells. And we have 12 cells in our antibody identification panel. Also , not sure what is "put up". What did you mean by "put up"? You putting something up, like up above something? Sorry, English is my 2nd language, I have a hard time understanding English sometimes. Thank you so much for your time and valuable knowledge. -
Anti-D + patient's red cells : 4+
-
error