
Everything posted by mollyredone
-

-
From my understanding, liquid plasma is plasma that has never been frozen and has a much longer outdate. We order it specifically from our supplier.
-
That's my understanding. We did label validation when we got plasma frozen < 24 hours, since it is labeled as thawed plasma.
-
I had trouble with the HemoTemps turning as well. We put them on our emergency release units when we set them up. Safe-T-Vue works well (as long as you don't put your thumb in the middle!) and we only use them on emergency release/massive transfusion and when we issue more than one unit at a time, so the cost really isn't an issue-$1.50 vs $1.
-
Malcolm, What was even more amazing was that they reviewed every transfusion and it was a rare one that didn't meet criteria! Simply amazing! But blood bank really can't review these deaths if there was no transfusion reaction called and no post specimen to work with and we don't know that the patient has even died. What can we do?
-
Mabel, I read on another thread from a couple of people at the reference lab that they were able to get negative antibody screens in tube with LISS. I tried that on one of our patients (we only have 2 so far) that had a positive screen in gel and was sent out for DTT treatment with no antibodies found, and the tube screen was negative. We did not read at 37. I had gotten a pre-treatment specimen and antigen typed it for all anti-sera we carry (Fy, Jk, K, S, C, c, E, e). If you do a LISS screen and it's negative, you don't have to give phenotype-matched products since nothing was destroyed. You don't do that with regular patients, right? I even emailed our reference lab, since technically these patients would be eligible for EXM with no history of an antibody, but I think I'll stick with IS XM. So, post-treatment screen in gel, if positive, screen in tube, if negative, do IS XM.
-
We just consider the units issued unless we are notified by the hospital they were transferred to. Many times they use it en route, or don't keep it stored properly, so the hospital won't accept it. I will sometimes call and ask if I know where the patient has been transferred. If they accept the products then they put them in their inventory and I change the status of the units to transferred.
-
Thanks everyone! I have emailed the QI coordinator. Who in your hospital investigates causes of death and decides whether the transfusion contributed to the patient's demise? Since most of the time there was no transfusion reaction initiated, I wouldn't even know that the patient had passed, unless I happened upon it.
-
If a patient has a transfusion within 72 hours of death, what is the proper workup? I've mentioned it several times to my medical director, but she is unsure of whether it has to be investigated. I don't get notices when a patient is deceased (although probably I could get a list) to be able to follow up on it. Would the pathologist just look at the patient's report and other comorbidities and decide the transfusion didn't cause the death? I saw a QI report from years ago where nursing investigated such deaths and decided they were not transfusion related, so I don't know if they reported the deaths to the FDA. Thanks!
-
That's what we do as well.
-
No I don't. Where does she work?
-
I am planning to retire the end of January. My hospital has just posted my position on their website. www.mercyrose.org The hospital is located in Roseburg, Oregon, which is 3 hours south of Portland and 1 hour from the coast. I would be happy to supply any other information about the community (about 25,000) and position if you are interested.
-
I am planning to retire the end of January and my hospital has just posted my position. If anyone is interested in the Pacific Northwest, I am located in Roseburg, Oregon, 3 hours south of Portland and 1 hour from the coast. The position is posted on mercyrose.org and I would be happy to answer any questions about the community or job.
-
We use manual gel for AHG crossmatches (not IS). Our procedure states that the computer will detect ABO incompatibility. The only time we would add an IS XM is during computer downtime. We have not been cited for this. "Under certain circumstances, a transfusion service may elect to omit the antiglobulin phase of the serologic crossmatch. The antiglobulin test may be omitted if the antibody screen is negative and there is no history of detection of unexpected antibodies. Nevertheless, a procedure to demonstrate ABO incompatibility, either a serologic crossmatch or a validated computer system, is required. The computer crossmatch may not be used if the patient has, or has had, evidence of clinically significant alloantibodies. Typing, screening and crossmatching of neonates can be abbreviated if a specific procedure is available. TRM.40650
-
-
We got cited on this for not running negative controls on Anti-A, Anti-B and Anti-AB, but I challenged it because it states "including a check against know positive and negative cells or antisera, or manufacturer's instructions for daily quality control are followed." The citation was removed.
-
We are doing our first CAP J survey with electronic crossmatching. I have a question about the second type and type on the units. The spaces show a place for forward and backward type on both the specimens and units. We only perform a forward type on our second type and units. Does anyone else do it this way? Will CAP mark us down if we don't fill in the other places? I also have to work with IT to let us add products to our proficiency samples, since they are entered differently, under proficiency samples. Or is that treating PT samples differently than patients?? Thanks!
-
The way I read this, is "if discrepancies exist". Not if discrepancies existed (in the past). So if you have a discrepancy and resolve it, it does not exist anymore. So if you can't resolve the discrepancy currently with other techniques, a serologic crossmatch would be required, but if you followed through with your procedure to resolve the discrepancy, it is no longer a discrepancy.
-
Now my problem is that it only allows a 24 hour expiration, and we make all our thawed plasma into 5 days from the start. I'm not a whiz on Hematrax. Thanks!
-
-
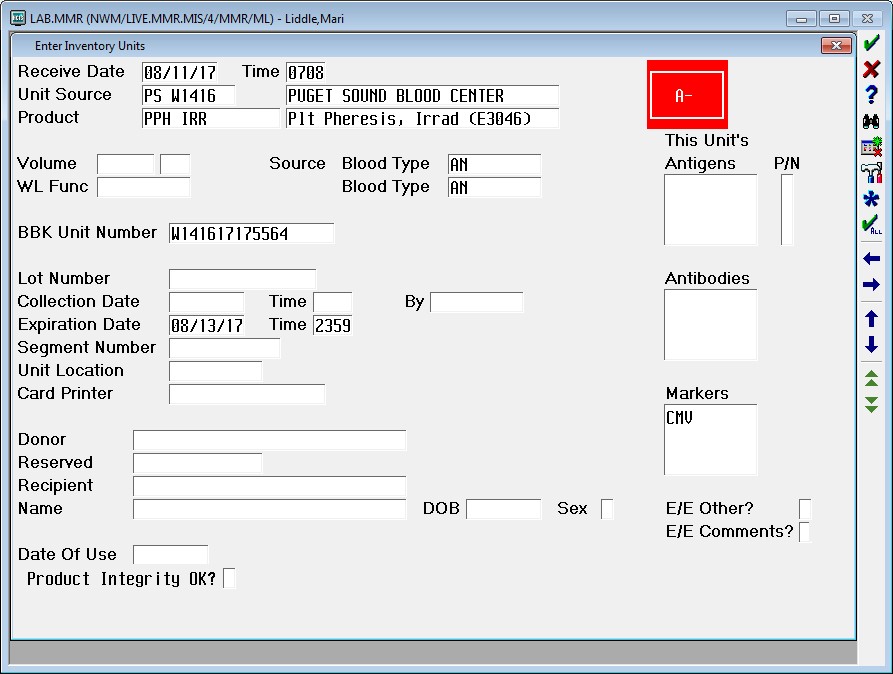
AuntiS, here's a screen shot of our enter units. The only difference is at the bottom under date of use. We have "product integrity OK?" and it is a required field. My IT guy says he thinks it is an NPR from Meditech. Maybe they have to do it, unless you have an IT guy that knows a lot about Meditech.
-
AuntiS, we have magic also, 5.67, but the field I mentioned has been there for a long time. How do you do a screen shot? I can get it in a word document, so I could just attach it, but I wanted to paste it directly.
-
I'm not sure how ours is set up differently, but we have to enter a Y or N on "product integrity OK?". We can't get past it, like the volumes on FFP or PPH. I could ask our IT guy if he knows how to make it mandatory.
-
Yes, we charge for all units, positive or negative, we type looking for antigen negative units. Obviously we don't type 10 units to find 1 K-negative unit, but base the number typed on the compatibility percentage. We are lucky to have a historical antigen database from our blood supplier, but sometimes we have to "wing" it and just grab a bunch from the shelf and type away!
-
Same here, but we only do about 400 a year and I have bigger fish to fry!


