Leaderboard

Popular Content
Showing content with the highest reputation since 07/20/2024 in all areas
-

anti-Jka likes to react unpredictably?
jshepherd and 2 others reacted to Malcolm Needs for a topic
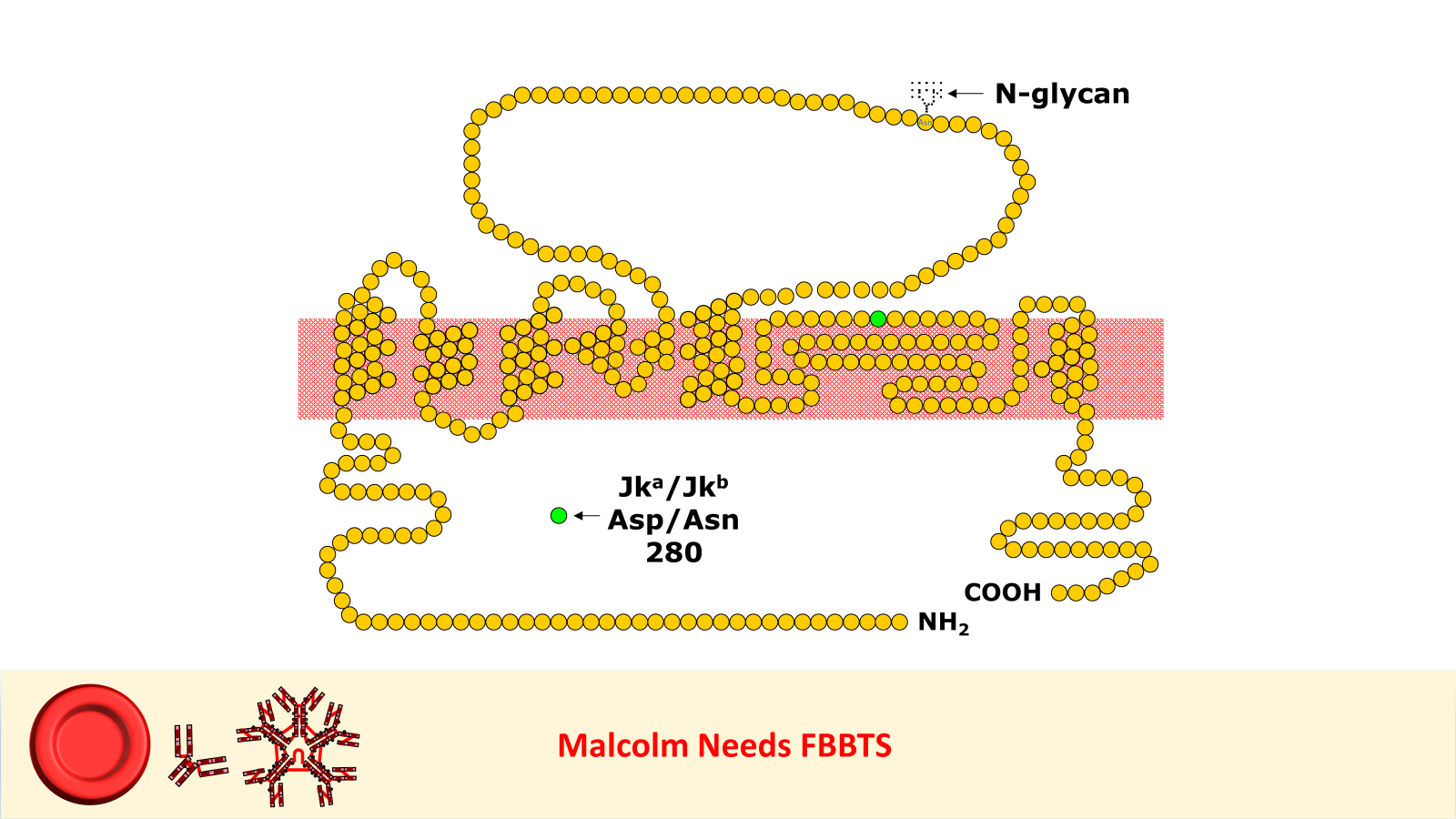
I worked in Red Cell Immunohaematology for most of my 43 years before retirement, including two times at the International Blood Group Reference Laboratory (IBGRL), and for over a decade at one of the NHS Blood and Transplant Centres in London. During that time, I saw some pretty weird Kidd antibodies, but never came across an example of one that reacted with red cells with Jk(a) heterozygous expression, but not with Jk(a) homozygous expression. One such "weird" type (although I never saw one) was the extremely rare, dominant inhibitor type In(Jk), similar, but, of course, not identical to In(Lu). These red cells usually type as Jk(a-b-), but their true Kidd type can be ascertained by Adsorption and elution tests.. These red cells are also more resistant to haemolysis by 2M Urea than red cells with "normal" expression of the Kidd antigens, but less resistant to haemolysis by 2M Urea than true "amorphic" Jk(a-b-) red cells. There are approximately 14, 000 copies of the Kidd carrier molecule per red cell (quite a small number, when compared with some other carrier molecules, such as the D antigen). The amino acid residue that defines either the Jka or Jkb antigens is very close to the red cell membrane in the 4th extracellular loop but is largely “hidden” by the 3rd extracellular loop (steric hindrance). Both facts may contribute to the weak reactions between Kidd antibodies and Kidd antigens. Schematic of the Kidd carrier molecule (after Wester ES, Storry JR, Olsson ML. Characterization of Jk(a+weak): a new blood group phenotype associated with an altered JK*01 allele. Transfusion 2011; 15: 380-392. DOI: 10.1111/j.1537-2995.2010.02795.x. In this paper, Wester et al also describe weakened forms of both the Jka and the Jkb antigens, but in each case, the amino acid substitution is remote from position 280 of the mature protein. In addition, an individual with the Trp171Arg mutation with weak Jk(a) expression has produced an anti-Jk3 or anti-Jk3-like antibody, and so they may be “dangerous patients” (Whorley T, Vage S, Kosanka J, Lose SR, Sandquist AR, Copeland TR, Westhoff CM. JK alleles associated with altered Kidd antigen expression. Transfusion 2009; 41 (Suppl.): 48A-49A (abstract). Lastly (for now anyway!), most foetal red cells sensitised by maternal antibodies react only with anti-IgG, but I (and a colleague Grant Webb) have both noticed, but not published, occasions when such red cells also react with anti-C3d and, in one case, only anti-C3d (see genuine photographs below).. 3 points
3 points -

MaxQ MTP Coolers 3.0
Marilyn Plett reacted to kjaggers1 for a topic
Good morning, Blood Bankers. I work at a Level 1 Trauma center and we just purchased 4 of these coolers. Has anyone had a successful validation plan? If so do you mind sharing. TIA. I am trying to find the most efficient way to validate and make sure we are covering every extreme possible.1 point -

anti-Jka likes to react unpredictably?
JasonS reacted to Neil Blumberg for a topic
Yes. And worse, some cells react differently, including having no reactivity, as compared with cells of the same degree of zygosity. Thus the possibility of Kidd antibodies needs to be seriously considered when the recipient is negative for one or both antigens and the panel is reactive but without clearcut specificity for Jka or Jkb.1 point -
No worries, any questions are helpful.1 point
-
I just answered this question. My Score PASS1 point
-
They can't all be hard. Also, as a reminder, I could really use help with new questions, I have a very small reserve.1 point
-

What's a high frequency antigen that might be weakened on expired reagent cells
jtemple reacted to Mabel Adams for a topic
We had to purchase a set of screening cells from a different vendor for DTT treating cells for Darzalex patients because when we validated it, the Duffy antigen we were testing didn't survive the process consistently. It was fine on Alba cells but not on Immucor cells.1 point