Leaderboard
-

Neil Blumberg
MembersPoints279Posts -
Malcolm Needs
Supporting Members ☆Points8,962Posts -
-




Popular Content
Showing content with the highest reputation since 07/06/2025 in all areas
-
Maternal alloantibody, not detected in baby - how long for antigen negative units
Darin and one other reacted to Neil Blumberg for a post in a topic
2 pointsThanks Malcolm. Never say never :).2 points -
Maternal alloantibody, not detected in baby - how long for antigen negative units
Yanxia and one other reacted to Malcolm Needs for a post in a topic
2 pointsArndt PA, Garratty G, Marfoe RA, Zeger GD. An acute haemolytic transfusion reaction caused by an anti-P1 that reacted at 37 degrees C. Transfusion 1998; 38(4): 373-377. DOI: 10.1046/j.1537-2995.1998.38498257376.x. Smith D, Aye T, Er LS, Nester T, Delaney M. Acute hemolytic transfusion reaction due to anti-P1: a case report and review of institutional experience. Transfus Med Hemother 2019; 46: 381-384. Published online as DOI: 10.1159/000490897. Irani MS, Figueroa D, Savage G. Acute hemolytic transfusion reaction due to anti-Leb. Transfusion 2015; 55: 2486-2488. DOI: 10.1111/trf.13178. Delk AA, Gammon RR, Alvarez H, Benitez N, Bright F, A hemolytic transfusion reaction caused by an unexpected Leb antibody. Laboratory Medicine 2021; 52: 303-306. DOI: 10.1093/labmed/lmaa070.2 points -
K Neg units requested for patient with autoimmune aplastic anemia
Neil Blumberg and one other reacted to kjmiller for a post in a topic
2 pointsGood morning, Malcom. Thanks for your reply- she is 61 yrs old and KNeg. I agree also with your approach, but we also have lots of patients with chronic anemias on transfusion support for whom we aren't giving K Neg. Maybe the dr. is just being more proactive in this case.2 points -
Maternal alloantibody, not detected in baby - how long for antigen negative units
Darin reacted to Malcolm Needs for a post in a topic
1 pointLove that!1 point -
Maternal alloantibody, not detected in baby - how long for antigen negative units
Malcolm Needs reacted to Neil Blumberg for a post in a topic
1 point"I'm sorry Neil, but Geoff Daniels quotes some HTR's caused by anti-N reacting at 37oC," These are, if I remember correctly, fairly ancient reports and I have never seen nor heard of a case of hemolytic transfusion reaction or HDFN due to anti-N despite having had hundreds of patients with anti-N in our service over the last half century. I've never heard of anyone else seeing one. So this is very possibly a case of old reports of hemolysis due to other causes (undetected antibodies for example). Methodology for antibody detection in the 1940s and 1950s, and even 1960s, was significantly less sensitive and accurate than currently. There are reports mentioned in Mollison and other comprehensive texts such as Daniels of hemolytic reactions due to antibodies (e.g., anti-P1, anti-Leb, etc.) that have never been reported in modern literature (the last 30-40 years). This makes me suspicious that these old reports are mistaken as to the cause of hemolysis. If the mother has an anti-N and the infant is not hemolyzing, and the antibody is undetectable I would not transfuse N negative blood. If the infant is hemolyzing, that is another story, obviously. A positive DAT, hemolysis and anti-N in the mother would dictate prudence and transfusing N negative blood. But I will stand by my original comment, which is that anti-N almost never causes clinically significant hemolysis in transfusion recipients nor in affected fetuses. Absent clinical and laboratory evidence for anti-N causing the infant's anemia, there is no reason to transfuse N negative blood when the antibody is not detectable in the fetus/infant.1 point -
ChemLabTalk: Biuret method
Malcolm Needs reacted to Cliff for a post in a topic
1 pointThat's OK. Pass (yay!) or fail, either way, it's always a learning opportunity.1 point -
Maternal alloantibody, not detected in baby - how long for antigen negative units
Yanxia reacted to Malcolm Needs for a post in a topic
1 pointI'm sorry Neil, but Geoff Daniels quotes some HTR's caused by anti-N reacting at 37oC, and one case of mild HDFN in a M+ N+ baby, where the mother was M+ N-, S-, s- Uvar, in the third edition of his book, Human Blood Groups.1 point -
Maternal alloantibody, not detected in baby - how long for antigen negative units
John C. Staley reacted to Neil Blumberg for a post in a topic
1 pointAnti-N does not cause hemolytic Transfusion reactions nor hemolytic disease of the newborn and fetus. So I would not give N negative blood in general, nor if the cross match is negative.1 point -
Maternal alloantibody, not detected in baby - how long for antigen negative units
Neil Blumberg reacted to John C. Staley for a post in a topic
1 pointCouple of questions for clarification. What is the specificity of the known Alloantibody? "Baby is born and our testing shows negative antibody screen." Was this AB screen done on mom or baby? If on the baby, was a current ab screen performed on mom and if so what was the results? Was a DAT performed on the baby? If so, what was the result? If not, why not? Thanks1 point -
Maternal alloantibody, not detected in baby - how long for antigen negative units
Neil Blumberg reacted to Cliff for a post in a topic
1 pointThis is an "older" policy as I am no longer with this organization, but we have a large delivery unit and a 50+ bed level I NICU. Here was our crossmatch policy for babies.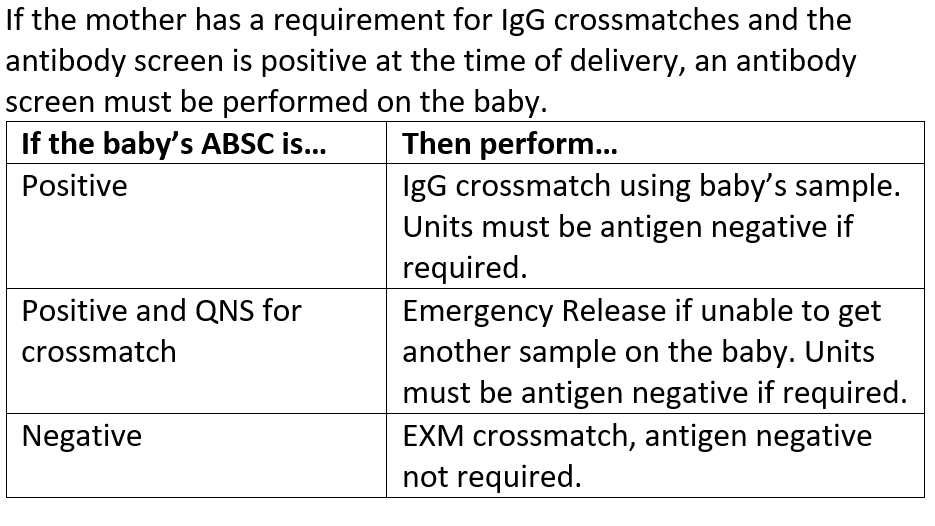 1 point
1 point -
Plasma transfusions
psykobillys reacted to Neil Blumberg for a post in a topic
1 pointAlso, were any of the transfused units antigen positive? This is the quickest way to get a negative indirect antiglobulin test ;).1 point -
1 pointI was the safety officer in my lab for over 10 years, and the thought of having to empty a blood bag gives me the shivers! Just too much opportunity for a splash and exposure, never mind the mess. Also, with tubing and hard plastic connectors attached to the unit, it really should be in a hard sided container. The connectors (we also call them spikes) could easily poke through a plastic bag alone.1 point

