

Malcolm Needs
Content Type
Store
Profiles
Forums
Blogs
Events
Frequently Asked Questions
Gallery
Downloads
Glossary
Links Directory
Questions
Jobs
Vendors
Posts posted by Malcolm Needs
-
-
I'm sorry, but I just don't believe the member who says they are 122 (Oh, I dunno though - I've just looked in the mirror!!!!!!!!!!!!!!!!!!!!).
-
Welcome to this wonderful site natalieelmquist. Enjoy.
-
Welcome to this wonderful site Liesel Nelson. Enjoy.
-
Welcome to this terrific site sshawkat. Enjoy.
-
Welcome to this wonderful site ashrafmusa. Enjoy!
-
Welcome to this GREAT site bbguy. Enjoy.
-
Most certainly, you need to have a thorough transfusion history on the patient, as my good friend Yanxia says above, but it also depends upon the condition of the patient. If the patient is exsanguinating, the old adage comes into play that it is not a medical triumph to give perfectly compatible blood to a corpse, when, in very many cases these days, a haemolytic transfusion reaction can be treated. HOWEVER, it is ALWAYS a decision to be made by a medically qualified person, rather than a laboratory qualified person to make, as to how urgent the transfusion may be.
IF there is time, it is always worthwhile doing a few more investigations. For example, is the patient DAT Positive, and, if so, is it IgG, IgM, IgA (rare), complement or a combination? Is the reaction seen in the auto-control due to a "cold" auto-antibody, or something else.
To repeat what I wrote above, it MUST always be a decision for a medically qualified person, rather than a "lab rat" (HATE that term, but I hope you know what I mean, without taking offence - being a retired "lab rat" myself), but, if it was a case with which I was dealing, apart from doing a few basic tests (see above) I would be happy to give the blood - and more importantly, receive the blood, if I were the patient. -
Welcome to this wonderful site Beginner. Enjoy and learn lots!
-
Welcome to this amazing site CLSKD. Enjoy.
-
Welcome to this fantastic site Jheimonen. Enjoy.
-
Welcome to this marvellous site Echo. Enjoy.
-
5 minutes ago, jshepherd said:
RhIg after giving 12 Rh pos units is futile. The patient will either make anti-D or not, too late to prevent at this point without exchange transfusion, which seems like overkill. We always say the female of childbearing age has to live in order to worry about anti-D in a future pregnancy, so we worry about that first.
")
Our policy is to revert to the patient's actual type after a massive situation. We would give A neg. Now, if the patient starts massively bleeding again, we would revert to A pos. Until the patient makes that anti-D of course.
Even though you've already given Rh pos to this patient, you did it during a mass transfusion, which is physiologically different than tranfusing an Rh pos unit low and slow.
I agree entirely, EXCEPT, we should think of females of child bearing POTENTIAL, rather than child bearing AGE. Think, for a moment, of a female who is group A, D Negative, who is, for example, 11 years old. Sorry to be picky, but, so often, these female children do not get the anti-D immunoglobulin they should be given.
- Cliff, jshepherd and John C. Staley
-
 3
3
-
Welcome to this fantastic site Marie Cannon. Enjoy.
-
Welcome to this fantastic site Demet Hazal Gomak. Enjoy.
-
Welcome to this fantastic site Jenny Hoek. Enjoy!
-

Who is this lady, and why did she win fame with regard to the genetics of the Rh Blood Group System?
-
7 hours ago, Antibodiesrock said:
I heard a lecture a while back, and I can’t find my notes, but I believe this could be the Er blood group system

Absolutely spot on. Well done!
See Karamatic Crew V, Tilley LA, Satchwell TJ, Al Subhi SA, Jones B, Spring FA, Walser PJ, Martins Freire C, Murciano N, Giustina Rotordam M, Woestmann SJ, Hamed M, Alradwan R, Al Khrousey M, Skidmore I, Lewis S, Hussain S, Jackson J, Latham T, Kilby MD, Lester W, Becker N, Rapedius M, Toye AT, Thornton NM. Missense mutations in PIEZO1, encoding the Piezo 1 mechanosensory protein, define the Er red blood cell antigens. Downloaded from http://ashpublications.org/blood/article-pdf/doi/10.1182/blood.2022016504/1922096/blood.2022016504.pdf on 30th September 2022.
-
1 hour ago, MGM said:
Well, its a multi-pass protein blood group so could be RH; Diego, Lewis ruled out. Kidd would be lacking proteins for Kidd null. Just a guess.
I'm afraid not. Many of the Blood Group Systems are multi-pass proteins.
-
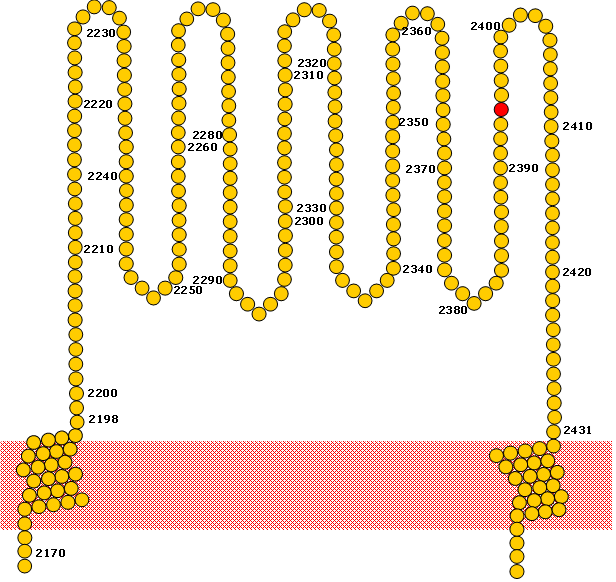
Okay then, here is another one.
A schematic of the showing the extracellular domain of the Piezo1 protein between amino acid residues 2198 and 2431.
WHat is the Blood Group System?
-
18 hours ago, Antibodiesrock said:
Another try… Jr(a)
Yep! See Reid ME, Lomas-Francis C, Olsson ML. The Blood Group Antigen FactsBook. 3rd edn, 2012, Academic Press. ISBN: 978-0-12-415849-8.
-
1 hour ago, donellda said:
I think it's Diego but I have been retired for a few years now and my mind is rusty (although this was my first thought)
No, I'm afraid not.
-
5 minutes ago, Antibodiesrock said:
I would say the H antigen

No, I am afraid not.
-
50 minutes ago, Melanie Oliveira said:
I'm going to go with Lewis antigen???
No, I'm afraid not.
-
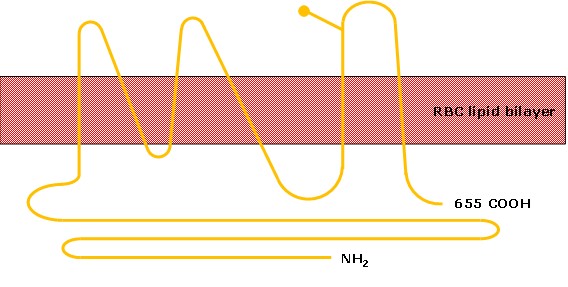
Here's one to start. This is a schematic of a molecule carrying a particular blood group antigen. The antigen is expressed on fewer Japanese individuals than most (but not all) ethnicities. What is the antigen?



Welcome Eric Parnell
in Introductions
Posted
Welcome.