All Activity
- Today
-
 test member joined the community
test member joined the community -
 In this case, it’s an anti-N, but I would have the same question (and potentially more important to answer) if this was an Rh, K, or other “more often significant” antibody. For clarity: mom: positive screen at referring hospital (we don’t have L&D) - anti N identified baby: got some blood at birth NICU, transferred to us. We get the record of anti-N from outside. Our tests show: baby negative ab screen, baby negative DAT We didn’t have anti-N reagent to antigen type baby (plus they had been transfused). I don’t remember precisely the hemoglobin, but it was in a range appropriate for transfusion - baby had undergone a few procedures with blood loss. There was very low suspicion for ongoing hemolysis and prenatal course had been okay - mom had been monitored by high risk MFM OB due to the antibody, but no intrauterine transfusions had been needed.
In this case, it’s an anti-N, but I would have the same question (and potentially more important to answer) if this was an Rh, K, or other “more often significant” antibody. For clarity: mom: positive screen at referring hospital (we don’t have L&D) - anti N identified baby: got some blood at birth NICU, transferred to us. We get the record of anti-N from outside. Our tests show: baby negative ab screen, baby negative DAT We didn’t have anti-N reagent to antigen type baby (plus they had been transfused). I don’t remember precisely the hemoglobin, but it was in a range appropriate for transfusion - baby had undergone a few procedures with blood loss. There was very low suspicion for ongoing hemolysis and prenatal course had been okay - mom had been monitored by high risk MFM OB due to the antibody, but no intrauterine transfusions had been needed. -
 Could I ask why? The ab would be passive, if the screen is neg, and this test would take days to come back, what is the value? Not saying you're wrong, just trying to learn.
Could I ask why? The ab would be passive, if the screen is neg, and this test would take days to come back, what is the value? Not saying you're wrong, just trying to learn. -
 I just answered this question. My Score FAIL
I just answered this question. My Score FAIL -
 All great questions, but I would also ask, what is the baby's Hb/Hct requiring a transfusion, and why not test the baby's DNA for the gene encoding the antigen cognate to the maternal antibody?
All great questions, but I would also ask, what is the baby's Hb/Hct requiring a transfusion, and why not test the baby's DNA for the gene encoding the antigen cognate to the maternal antibody? -
 I just answered this question. My Score FAIL
I just answered this question. My Score FAIL -
 Couple of questions for clarification. What is the specificity of the known Alloantibody? "Baby is born and our testing shows negative antibody screen." Was this AB screen done on mom or baby? If on the baby, was a current ab screen performed on mom and if so what was the results? Was a DAT performed on the baby? If so, what was the result? If not, why not? Thanks
Couple of questions for clarification. What is the specificity of the known Alloantibody? "Baby is born and our testing shows negative antibody screen." Was this AB screen done on mom or baby? If on the baby, was a current ab screen performed on mom and if so what was the results? Was a DAT performed on the baby? If so, what was the result? If not, why not? Thanks -
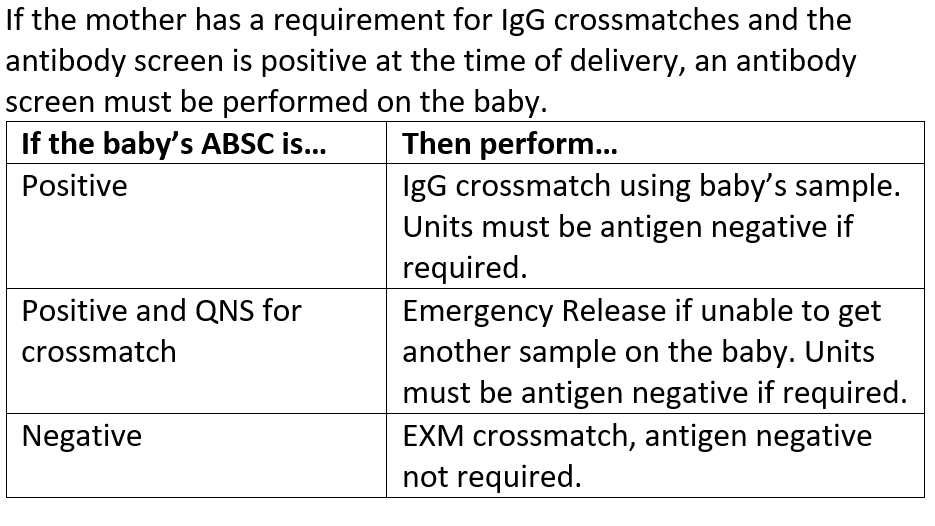
This is an "older" policy as I am no longer with this organization, but we have a large delivery unit and a 50+ bed level I NICU. Here was our crossmatch policy for babies.
-
I'm a little newer to the blood bank, so often need help understanding / reconciling our current policies - appreciate any help or insights (or references!) Situation: Mother has known alloantibody (a potentially clinically significant one). Baby is born and our testing shows negative antibody screen. Our current policy requires antigen-negative units for transfusion (with resultant AHG crossmatch) if maternal alloantibodies are present, but it doesn't say HOW LONG we need to give those antigen negative units. Questions: Is the use of the antigen negative units in this neonate with no detectable antibodies (negative screen) because of the possibility of "missing" low titers of maternal antibodies in baby? [I'm having trouble finding the REASON for this practice] Am I correct in thinking that we could antigen type the neonate, and if we prove they lack the antigen in question then we could drop the requirement. [the baby in the actual case that brought this up had been transfused at the birth hospital, so we didn't attempt this] How long does this antigen-negative requirement stand? Right now, our policy is being interpreted as lasting until the baby is 4 months old, but I really am not sure where that came from.
-
 I just answered this question. My Score PASS
I just answered this question. My Score PASS -
 I just answered this question. My Score FAIL
I just answered this question. My Score FAIL -
 I just answered this question. My Score PASS
I just answered this question. My Score PASS -
I just answered this question. My Score PASS
-
I just answered this question. My Score FAIL
-
I just answered this question. My Score FAIL
-
 I just answered this question. My Score FAIL
I just answered this question. My Score FAIL -
I just answered this question. My Score PASS
-
 Happy Birthday!🎂
Happy Birthday!🎂 -
I just answered this question. My Score PASS
-
 I just answered this question. My Score FAIL
I just answered this question. My Score FAIL -
 I just answered this question. My Score FAIL
I just answered this question. My Score FAIL -
 I just answered this question. My Score FAIL
I just answered this question. My Score FAIL -
 I just answered this question. My Score FAIL
I just answered this question. My Score FAIL -
 I just answered this question. My Score FAIL
I just answered this question. My Score FAIL -
Virus This question and answer was originally published on Lab Tests Guide. They have generously permitted us to repost here on our site. This site's admin may have slightly modified the questions and answers. Please consider visiting their site: https://www.labtestsguide.com/ Submitter Cliff Category General Lab Submitted 07/02/2025
-