Everything posted by Dansket
-
 At this point in time, there is only one panel available for Wadiana. The software (and the gel cards ) is quite different I would ask for a demo from Grifols.
At this point in time, there is only one panel available for Wadiana. The software (and the gel cards ) is quite different I would ask for a demo from Grifols. -
-
Have been using and will continue to use TEMP-CHECK (albeit an older version) for years. We check units individually.
-
It would be interesting to know how reference labs (Quest, LabCorp, ARUP etc.) do antibody screens on prenatal specimens.
-
If they report it, investigate it. It the time frame is extreme, pathologist should put a note on the patient's chart.
-
Current regulations AABB, CAP, etc. do not permit use of a single pooled cell reagent for pretransfusion compatibility testing. Maybe on prenatals, but I don't used pooled cell for them either.
-
-
See page 6 of your product dictionary. I am puzzled as to why antibody screen results are being entered on paper and then in the computer. That process is almost guaranteed to set you up for failure. I'm using Meditech C/S 5.67. All results are entered directly into Meditech from the test tube or gel card, no paper! What's scary to me is that Meditech has been implemented at your site without anyone looking under the hood to see what's possible. Product Dictionary page 6.pdf
-
-
Yes. Our 5-Day plasma expires at 2359 on fifth day after thawing regardless of the time thawed.
-
-
I stopped "washing cord blood samples 3 times" over 20 years ago. Routine washing of cord blood red cells is a "solution" looking for a problem. If you have documented evidence in your facility that unwashed cord red cells produce a high incidence of false-positive test results, then wash, wash, wash. Otherwise, I would wash cord red cells only when a discrepancy is detected (positive Rh control test).
-
Yes, we do. We are a small facility that has standardized collection of blood samples for pretransfusion compatibility testing. All blood component requests require that a Type and Screen blood sample be collected within 3 days of the intended date of transfusion. We also use the TYPENEX Blood-Recipient Identification System.
-
Try a flow chart, or even a set of flow charts.
-
-
-
We will rule out C and E in the presence of anti-D with a single C+c+ or E+e+ cell. K may be also ruled out with a single K+k+ cell.
-
Yes, Nursing orders the Post-partum RhoGAM protocol on mothers known to be Rh negative (according to prenatal records) as well as mothers whose Rh type is not known. ER orders Antepartum RhoGAM protocol on females known or suspected of being pregnant.
-
In our facility, Nursing orders either the Post-partum RhoGAM protocol on the mother with the Cord Blood Workup on the newborn or the Ante-partum RhoGAM protocol. After completion of appropriate testing, Blood Bank automatically assigns RhoGAM syringe to mother (if indicated) and notifies Nursing the mother is candidate and RhoGAM syringe is ready for injection. This is a one step process for Nursing.
-
Are you creating a new product in your Meditech aliquot routine? Example: RBC>RBCaliquot or RBC>RBC (with reduced volume)? I believe Meditech will add a letter to the DIN to differentiate between the two components when you RBC>RBC (with reduced volume).
-
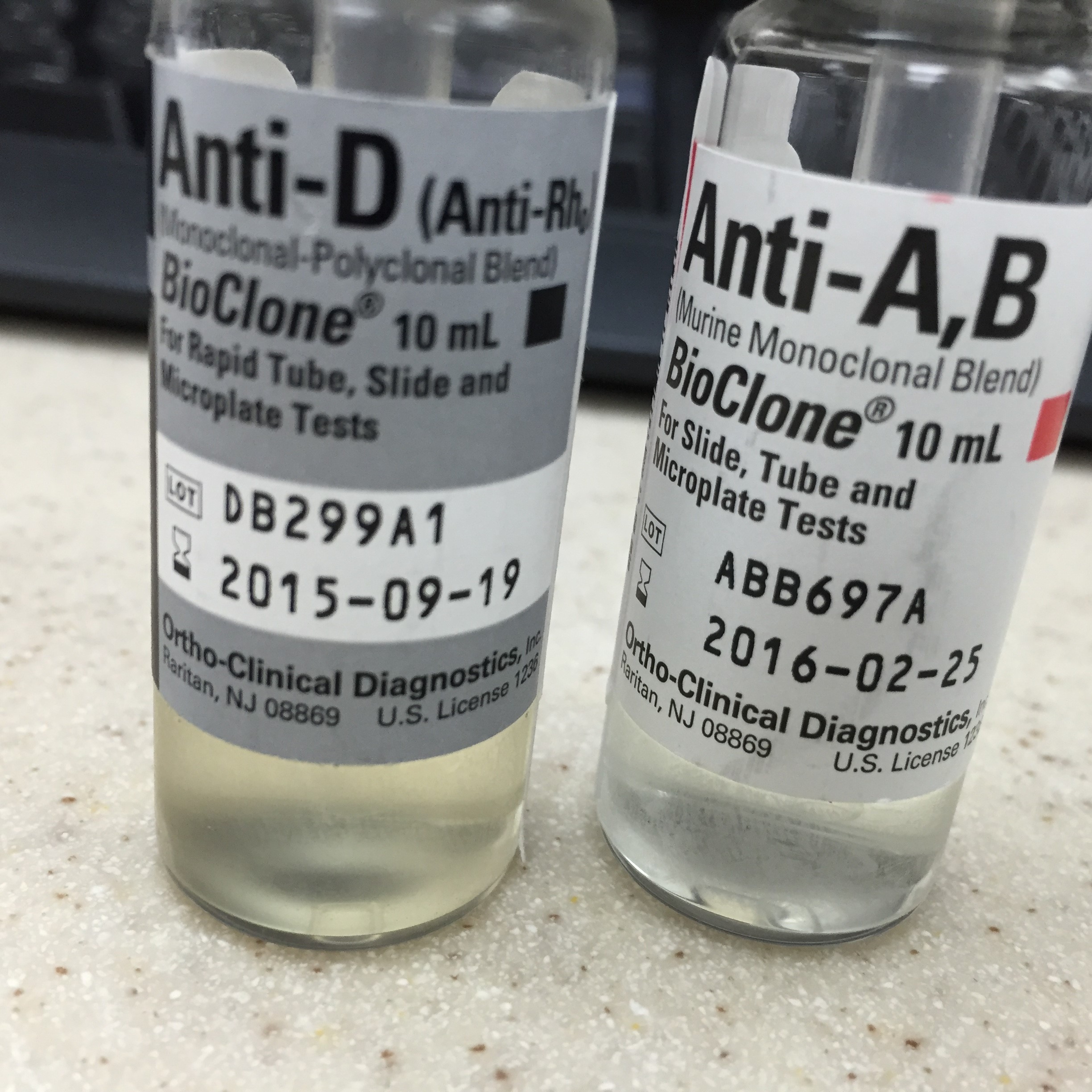
As neither anti-A and anti-B were detected by tube or gel in the patient's plasma and the patient's red cell genotype is AB, what is the appropriate blood group to select for transfusion?
-
As you know a "call box" can be created in the LIS Canned Text dictionary and its mnemonic can be entered as a "Result Comment" for T type tests in the BBK Test dictionary. Unfortunately, the BBK test "ABS" is unique (not a T test) and cannot be configured with a Result comment. I believe one option is to contact the Iactic company (iatric.com) and request a quote from their Report Writing service. Expect the cost to be => $1000. They can do some amazing things in Meditech. Or you can do what goodchild and I have done by reflexing an Order group.
-
Tube test is the best way to resolve ABO plasma grouping discrepancies when expected anti-A and/or anti-B not detected in Gel.
-
Our ProVue is not interfaced to LIS. We print ProVue 'Results by Sample' reports and then manually key results from report into Meditech. I believe that these reports can be considered "instrument printouts". What length of time should "instrument printouts" be retained. We are not AABB/CAP accredited.
-
We remove a donor unit number label from back of bag and affix to base of donor tubing inlet on the front of the bag. This visually identifies that unit ABO/Rh has been serologically confirmed (in case of Meditech downtime). In Meditech C/S 5.nn, crossmatch results (serologic or electronic) cannot be entered on a unit if ABO/Rh serological confirmation test results have not been saved and filed.