Malcolm Needs
Content Type
Store
Profiles
Forums
Blogs
Events
Frequently Asked Questions
Gallery
Downloads
Glossary
Links Directory
Questions
Jobs
Vendors
Everything posted by Malcolm Needs
-
 I'm afraid I still can't agree with this methodology, for a couple of reasons. Firstly, antibody/antigen reactions are, largely, governed by the Law of Mass Action. As a result, and given a steady state of conditions (e.g. temperature), however long the incubation time may be, once a state of equilibrium is reached, there will be no net gain of antibody coating antigens, however long the incubation time may be extended. Certainly, LISS will increase the rate of association of antibody and antigen enormously, but this will apply equally to the auto-antibody as any allo-antibody that may be present, however, of course, some antibodies will only react visibly with red cells that have homozygous expression of a particular antigen, and, if such an antibody is present, it will be very difficult to detect in the presence of an auto-antibody, but can still cause a haemolytic transfusion reaction, albeit, usually a delayed reaction, but it can still cause damage to the renal system in particular. For these reason, I would always perform an adsorption, to get rid of the auto-antibody, even if I had no intention of performing specificity tests on the auto-antibody (although, it goes without saying, I would go all out to try to ascertain the specificity of any allo-antibody detected). I am trying to write a book at the moment, called "Human Red Cell Serology and Blood Groups for Beginners", and Chapter 2 deals with Serological Techniques. I attach the draft copy, which also gives relevant references, the odd diagram and abbreviations I use throughout the various chapters. Chapter 2 Serological Techniques in Routine Blood Transfusion and Red Cell Immunohaematology Laboratories.docx Chapter 2 Serological Techniques in Routine Blood Transfusion and Red Cell Immunohaematology Laboratories Figures.docx Abbreviations.docx
I'm afraid I still can't agree with this methodology, for a couple of reasons. Firstly, antibody/antigen reactions are, largely, governed by the Law of Mass Action. As a result, and given a steady state of conditions (e.g. temperature), however long the incubation time may be, once a state of equilibrium is reached, there will be no net gain of antibody coating antigens, however long the incubation time may be extended. Certainly, LISS will increase the rate of association of antibody and antigen enormously, but this will apply equally to the auto-antibody as any allo-antibody that may be present, however, of course, some antibodies will only react visibly with red cells that have homozygous expression of a particular antigen, and, if such an antibody is present, it will be very difficult to detect in the presence of an auto-antibody, but can still cause a haemolytic transfusion reaction, albeit, usually a delayed reaction, but it can still cause damage to the renal system in particular. For these reason, I would always perform an adsorption, to get rid of the auto-antibody, even if I had no intention of performing specificity tests on the auto-antibody (although, it goes without saying, I would go all out to try to ascertain the specificity of any allo-antibody detected). I am trying to write a book at the moment, called "Human Red Cell Serology and Blood Groups for Beginners", and Chapter 2 deals with Serological Techniques. I attach the draft copy, which also gives relevant references, the odd diagram and abbreviations I use throughout the various chapters. Chapter 2 Serological Techniques in Routine Blood Transfusion and Red Cell Immunohaematology Laboratories.docx Chapter 2 Serological Techniques in Routine Blood Transfusion and Red Cell Immunohaematology Laboratories Figures.docx Abbreviations.docx -
In what way does a LISS screen with 30' incubation "CONFIRM" that there are no underlying clinically significant allo-antibodies present? I am always happy to learn.
-
Welcome to this fantastic group kastalia.
-
I've had further thoughts upon this case (having told you not to worry about it - I live a sad life - NOT!). It struck me that the patient has an Rh type of D+ C+ c+ E+ and e+, suggesting that the probability is that the patient has a genotype of DCe/DcE (R1R2), but this may not be the case. She could have one of the rarer Rh genotypes, such as DCE/Dce (RzRo), DCE/dce (Rzr), Dce/dCE (Rory), etc, and this may be potentially important. Some years ago, Joyce Poole explained to me that most grouping reagents labelled as anti-C are, in fact, a mixture of anti-c and anti-Ce, and this, she told me, included most monoclonal anti-C reagents (which surprised me, to be honest). This is because the vast majority of the red cells transfused that stimulate an anti-C would have the haplotype of either DCe or dCe, or both, and will, therefore, also stimulate an anti-Ce. As a result, these "hybrid" anti-C/anti-Ce reagents will react more strongly with red cells expressing the Ce compound Rh antigen (Rh7) and the C antigen (Rh2), than with red cells that only express the C (Rh2) antigen. This would not, incidentally, explain the stronger than normal reaction with the e antigen. However, if the patient does express one of the rarer Rh types mentioned above, say she is RzRo, she can actually produce an allo-anti-Ce, and most antibody panels only contain C+ red cells that are only Ce+ as well. In other words, her antibody in the plasma MAY be identified as an anti-C, whereas it is actually a monospecific anti-Ce, which would neatly explain why she has an apparent anti-C. Of course, she may also have an auto-anti-C, or a mimicking auto-anti-C (and, possibly, an allo-anti-Bg of some sort). Sadly, for a nerd like me, I doubt if we will ever know! I think it was John C Staley who once accused me of looking for zebras, when I hear horses hooves (I may be wrong, but I think it was John). Anyway, this proves that he was absolutely correct about me!!!!!!!!!!!!!!!!!!!!!!!!
-
I am a complete antibody nerd, but, in this case, I think that you would be knocking your head against a brick wall for no reward if you try to go any further with this one. My first thought was that it may be a case of an anti-hrB, but when I saw that the patient was a Caucasian, that was virtually "blown out of the water". Then I saw that she had a positive DAT with anti-IgG, but not anti-Complement, and I thought Rh specificity, and, like you, I immediately thought of a mimicking auto-anti-C. The problem is that, if you performed an elution, to actually PROVE that was the case, you would have to have access to some exceptionally rare Rh types (red cells that even many Reference Laboratories lack, let alone Hospital Laboratories). My mentor, Joyce Poole, who taught me so much, taught me (in no uncertain terms!) not to waste such rare red cells, when I was but a young whipper snapper at the International Blood Group Reference Laboratory when it was still in London - and I'm glad she did before her boss, Carolyn Giles, needed to teach me!!!!!!!!!!!! In this case, particularly as the patient is even older than am I, AND has been discharged, even as an antibody nerd, I would be inclined to let sleeping dogs lie!
-
Welcome to this wonderful site Constance Castro Dominguez.
-
Welcome to this wonderful site Pamo.
-
1 or 2-person check for plasma protein product
Malcolm Needs replied to TMGal's topic in Transfusion Services
When I was working on-call in a hospital laboratory, I was a lone worker. I gave out blood, blood components and blood products without anyone checking me, apart, of course, from the patient's own immune system! As far as I know, and I think I would, none of them had either an immediate or fatal haemolytic transfusion reaction. -
True, but the point is, to make this joke of a requirement worthwhile, rather than just a box ticking exercise, there should be specified specificities, but they won't do that because they know (or, rather, should know) that they could never get sufficient of "weak" antibodies of certain specificities, and that diluted "strong" antibodies will have a completely different association constant, and so using these diluted "strong" antibodies will serve to control/compare absolutely nothing.
-
Welcome to this wonderful site kjmiller.
-
Antibody and Antigen Reference Books
Malcolm Needs replied to kmmoton's topic in Education / Quality
It depends what you are after. The second edition is more about the serology of the blood groups and their respective antibodies, whereas the third edition included much more about the genes involved and how they can be tested. They are both superb books though. -
Antibody and Antigen Reference Books
Malcolm Needs replied to kmmoton's topic in Education / Quality
Sorry. I never did get back to this after my holiday. I still haven't come across a brilliant book on the subject, but four books I do like are shown below, and (sorry for being egocentric) so is one of my own lectures that touches upon the subject. Serological Techniques for Antibody and Antigen Identification.pptx
-
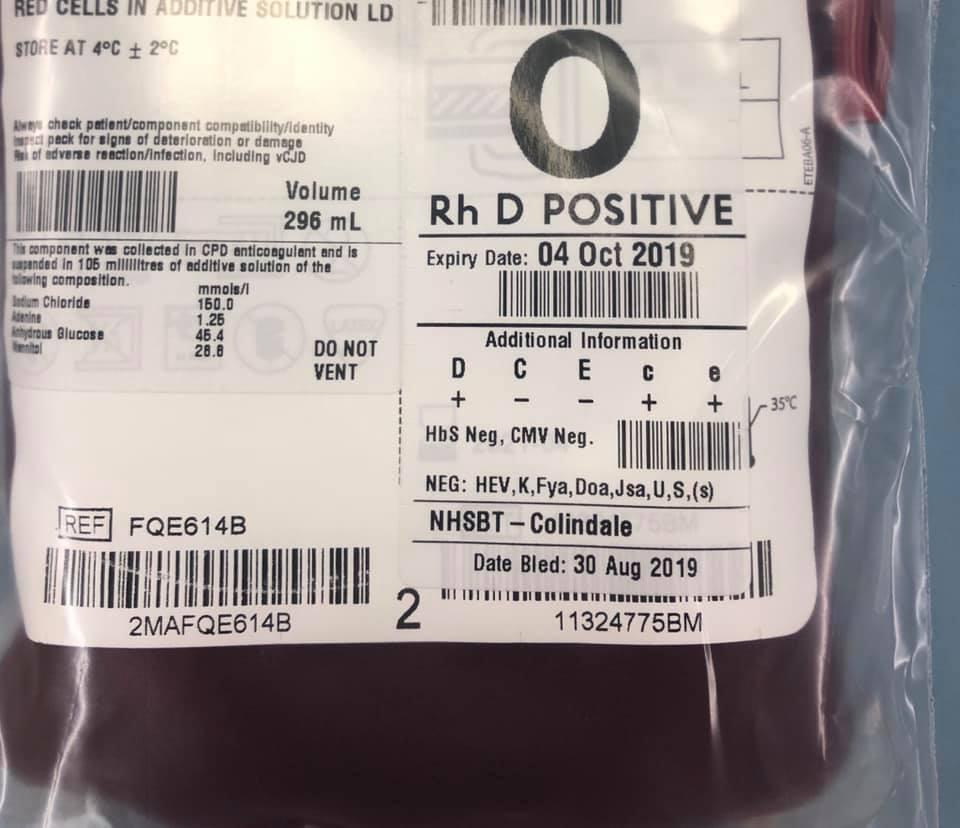
Thanks. Now I can see from where you are coming, and that all makes it plain, and I was being stupid! The problem is, in the UK, every unit has the Rh phenotype on the bag label (see the attached photograph), and I keep forgetting that is not the same in all countries (I am being parochial in my old age!).
-
Welcome to this wonderful group SWelsh.
-
May I ask if you are talking about positive controls or negative controls? The reason I ask is that, if you are talking about positive controls, you should not be using R1R1 or R2R2 red cells anyway, as they have homozygous expression of the C and e, and the c and E antigens (unless, of course, they are from a donor with a VERY rare type, such as R1/D-- or R1/Rhnull). Should you be using unit segments from a presumed R1R2 donor. On the other hand, if you are talking about negative controls, then even if you did find it easier to get r"r or r'r units, they, of course, would have heterozygous expression of the E and e antigens, and the C and c antigens, and so would be unsuitable for negative controls for those antisera. I'm sorry if I am sounding like I am trying to "teach my Grandmother to suck eggs" (and it is probably me getting entirely the "wrong end of the stick"), but I am totally confused.
-
QUITE RIGHT TOO!
-
So, this PROVES that CAP do not know the A from their elbow. ALL Blood Transfusion Reference Laboratory Staff, not to mention MOST Blood Transfusion Hospital Laboratory Staff KNOW that not all antibodies can, by any means, be detected by ALL serological techniques (saline, albumin, enzyme, LISS, IAT, inhibition tests, recombinant blood group proteins, etc), let alone by ALL technologies (glass, tube, plastic tube, liquid phase microtitre plates, solid phase microtitre plates, column technologies, etc), BUT THOSE WHO RUN CAP KNOW BETTER THAN EVERYONE. They should be thoroughly ashamed of themselves, and go back to kindergarten.
-
Welcome to this superb site Labrat54.
-
Welcome to this wonderful site Midna Torres.
-
Happy Birthday from someone else!
-
Meditech BB module and antibody screen reference range
Malcolm Needs replied to frenchie's topic in Transfusion Services
I may well be being very thick here, but what exactly is a reference range for an antibody screen? Is it how many positive results you would expect on samples from individuals who are new to your own institution? If it is, and I am not being completely stupid (I probably am), how can ANYONE possibly come up with such a range? Surely, such a range depends upon al sorts of different factors, such as sex (women who have been pregnant are almost bound to have more atypical alloantibodies than either women who have not been pregnant, or males (who have never been pregnant), individuals who have been multiply transfused because of such things as Sickle Cell Disease, or thalassaemia, but even then, the atypical alloantibodies detected in such individuals depends upon factors like how many transfusions they have received, whether the donors are of the same/similar ethnicity as the individual, and, indeed, whether or not the individual is a respondent or not (or, as the great Dr/Prof Ed Snyder once lectured the British Blood Transfusion Society (BBTS) concerning patient's who have a "virtual transfusion" (they are shown a photograph of a red cell and, as a result, form an atypical alloantibody). There are just so many variables, I cannot see how there could possibly be a "reference range", unless, as I suspect, I have got completely the wrong end of the stick/ -
Supervisor competency assessment
Malcolm Needs replied to Tympanista's topic in Accrediting Agencies
We did the same, back in the Dark Ages when I was still working. -
It is with huge regret that I can reveal that Marilyn Kay Grandstaff Moulds has just informed me that Peter Issitt died on Wednesday evening. One of the truly great blood groupers.
-
Welcome to this great group of people Mumiab.
-
Welcome to this great group Day.


.jpg.2e27e0988789c867310a9581d54c2e7f.jpg)