
Everything posted by Yanxia
-
 The mishandled ECMO can cause hemolysis. I know this can't happen in your hospital, just a little hint.
The mishandled ECMO can cause hemolysis. I know this can't happen in your hospital, just a little hint. -
In our lab, we do 30 patients ABO typing daily in average. In those tests we will find out forward and reverse typing mismatch at least once daily. Maybe because we tested patients' sample, the incidence is higher than donors', but just as Malcolm said it is definitely necessary to do forward and reverse typing and make sure they are matching.
-
Mabel, maybe there was an anti-P1 which was initially a cold reactive one that warmed off by 30 min prewarm technique. But I can't explain why it didn't react with reagent cells after transfudion except there were antigen loss.
-
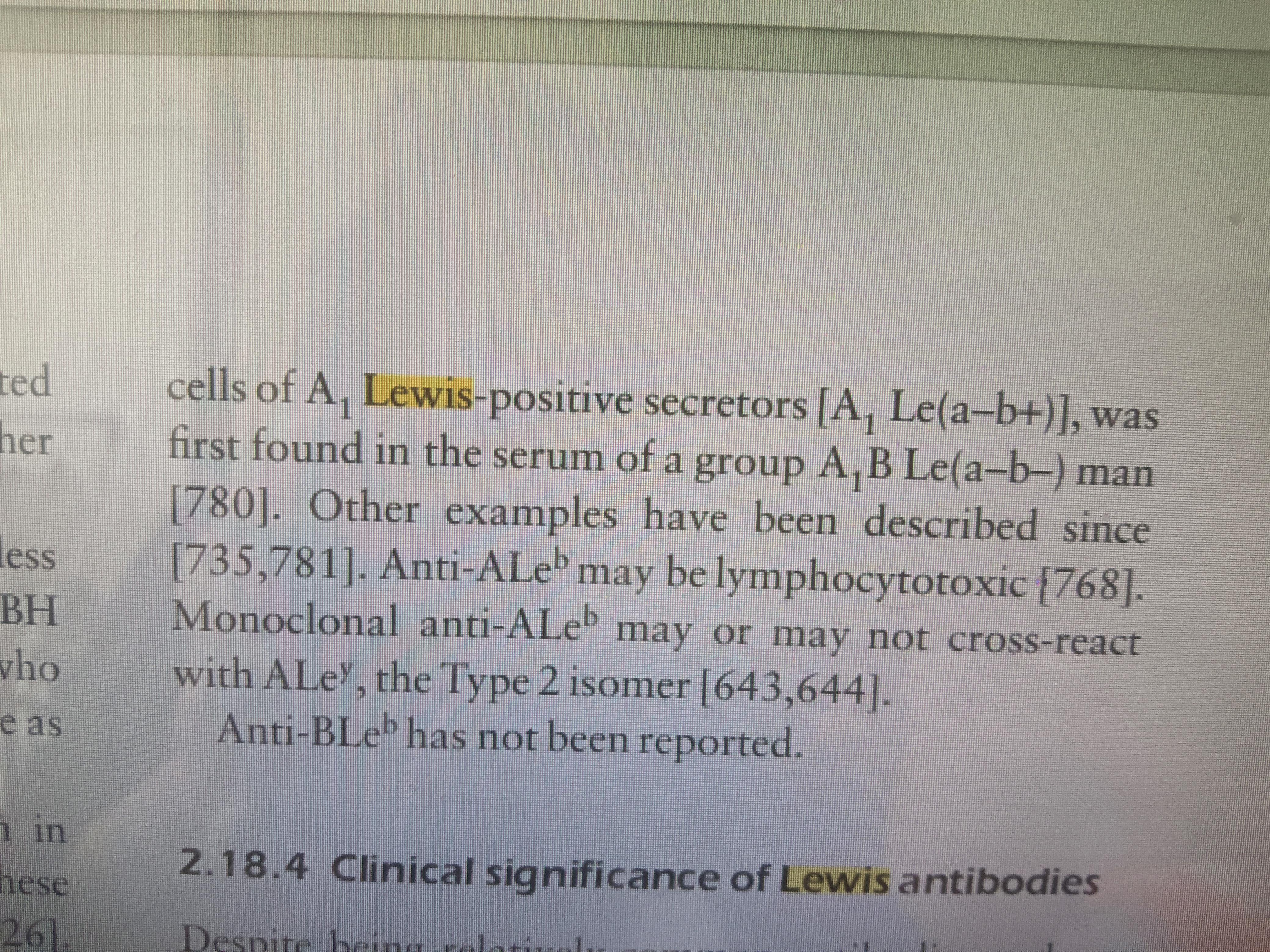
This is from Human Blood Groups, Deoff Daniels, the second edition.
-
Thanks Mabel for your explanation. I think we can exclude the protein factor. 1.In my work, I have noticed that the reagent cells express less H antigen than the donor cells do. Our screen and panel cells have 3-month shelf life, but our donor cells only have about 35 days. Even though we do our best to preserve the antigens on panel cells, there are still some losses. Of course, there are other antigen loss other than H. 2.I have read lewis antibodies may react with A type, sorry I can't recall it exactly, I will check it out after this work shift when I get home. If there is an anti-A Lewis antobody, it will react stronger with donor cells. As to the incompatible O donors, my bold guess is they express more Lewis antigen than reagent cells. Sorry again for my imagination.
My qustion may sound stupid, but out of passion, I still ask out. I am sorry for this. Did you test the after transfusion specimen against the reagent cells? I guess the pos reaction to antigen neg donors maybe caused by protein in the patient's blood sample.
Another tip: I remember there is a saying that the anti-A1 lectin is not so specifical against A1 antigen. Sometimes it will react weakly with A subgroups.
This is a very intersting case. As there is no transfusion history and leukemia, I prefer it is Chimera. Maybe we can test other red cell antigens such as the Rh system to prove or exclude it.
The elution react with the father's red cells. Using those three Rh types, I reference auto-antibodies adsorption, because I am not sure if there is a mix of anbodies in the mother's.
Maybe we can try by using the mother's serum to react with the father's red cells (if they are not ABO type compatible, using R1R1,R2R2,rr red cells adsorb the allo-antibodies separately before doing elution ). I am not sure if I can make myself clear.
I just can't understand why the phenotype gives 4+ of c antigen when the genotype is c neg.
Thanks for sharing, Andrea. I have spotted one big difference between your SOP and mine, that is we don't discard the pipette tips for each dilution. I will do paralle test to see the difference in titre later.
Maybe some day we can actually do it, My meaning was if we detected an antibody and didn't make sure it was auto or allo, we did crossmatch using a method that was sensitive, in case we missed it.
I guess the solid phase is more sensitive to detect the auto in this patient. I will use the same method as detecting the antobodies to do crossmatch. Of course I will do saline and AHG crossmatch as well. Just my humble opinion.
I am kind of curious about is the crossmatches and ABID using the same method?
I guess if there was carry-over it is the same as using the same tube during the whole washing process.
I mean the freezing and thawing test.
Would you explain it more specifically, please? It sounds new to me.
Is can detect anti-Vel which isclinical significant.
The elevated IgM in the baby means there was intrauterie infection.
It seems like allo- anti-I. But I can't explain why the Liss reaction is neg. I am waiting experts to explain and learn from them.
May you kindly give us more details about it? Is it about the ionic strength? Thank you.
Maybe repeat ABO typing can prove it.
It needs about 6 minutes to expel the substance in blood circulation through urine.

Important Information
We have placed cookies on your device to help make this website better. You can adjust your cookie settings, otherwise we'll assume you're okay to continue.