Everything posted by Lekota40
-
 My response to Mr. Staley's comment is that I indeed have been a supervisor. I was a "working supervisor" that spent a heck of a lot of extra hours at work to do my supervisor work after the regular. I kept current on every aspect of the lab-not just blood bank. I was actually the evening shift supervisor and had to deal with all the phlebotomy headaches as well. So what I'm getting at is that I feel "insulted" by the fact that I have to be supervised by those I feel dont even try to reach out to what "used" to be their world as a bench tech and give us some semblance of credit, knowledge and appreciation.
My response to Mr. Staley's comment is that I indeed have been a supervisor. I was a "working supervisor" that spent a heck of a lot of extra hours at work to do my supervisor work after the regular. I kept current on every aspect of the lab-not just blood bank. I was actually the evening shift supervisor and had to deal with all the phlebotomy headaches as well. So what I'm getting at is that I feel "insulted" by the fact that I have to be supervised by those I feel dont even try to reach out to what "used" to be their world as a bench tech and give us some semblance of credit, knowledge and appreciation. -
I work at a blood center and we have FDA inspections. We handwrite way more documentation than anyone wants to and passed with flying colors so not understanding the "no handwriting" item.
-
After getting a lot of great input and some bashing about how I should NOT criticize my superiors-which will not do here the opinion I seek is the following: Should a person NOT actively working the bench be allowed to review and approve a tech's work? You may have book knowledge but your hand's on experience is not there. I sort of present another scenario would you want a doctor that hasnt operated in 5 years supervising a new surgeon or a person that owns a car repair shop that was a mechanic and reads the latest and greatest but hasnt worked on any new model car in 5 years repair your brand new newest car model? I feel current 'hands on" knowledge can far exceed "book knowledge".
-
Love all these replies! My 2 funniest and scariest (do to wondering where the knowedge levels of RNS and MDs are sometimes) was the nurse that came down in the middle of the night to pick up blood on a B pos patient. We crossmatched B Neg as the units were shortdated and we wanted to not waste them as there is many less B neg that B pos patients. She questioned up and down the "wrong blood type" I explained to her the whole its perfectly fine to transfuse Rh neg blood to an Rh pos patient just dont do it the other way. Showed her a blurb in the technical manual stating such as well. She took the blood and returned in about 15 minutes saying there was no way she could give this blood to the patient. Ended up having to call the pathologist on call at like 2 am to explain it was perfectly fine to her and since it was a doctor explaining it she finally took it. The other scenario is the patient they took to the OR and drew a crossmatch specimen while the patient was on the table that ended up with an antibody. The tech working it up kept trying to explain the delay and the doctor said "well just give me O negative".
-
cimergen and anne that commented on my venting on this forum about my superiors I thank you for your coments and concerns. I will refrain from doing so in the future. What would you recommend as an alternative? Not trying to be coy here looking for serious constructive criticism. I really have had a bad time lately with my job as have coworkers working under the management we have and anytime we attempt to address it with HR or others over them we are dismissed as it being "our" problem and attitude. Understandably that could be an arguent tor management if one 1 or so people were complaining but when pretty much everyone in a department does that to me shows something should be addressed. I have been in supervision so I know that end of the scope and I at least attempted to listen to people and admit when I was wrong.
-
I have addressed issues with my superiors with HR etc it has got me nowhere. So why do I continue to work there you may ask? I do because I like what I do and do believe I do it well and jobs as a Med Tech where I live are limited and I cant move. The "bashing" as you call it in a public forum is a serious stress reliever and since I do not and will not mention names I'm not really harming anyone. I am I guess attempting to point out the fact that those in charge of us are NOT always the best qualitfied. It would be nice to have to take some sort of test to qualify and have unbiased HR personal but real world is that doesnt happen.
-
Here's the scenario. I work both at a blood center which serves as a reference lab to smaller hospitals primarily for antibody IDs and also at a trauma center which is a constant unknown as far as how much multitasking you need to do in order to provide the best patient care in blood bank. I agree in that being human we can make mistakes but I'm sure all of us do multiple checks, even while rushed to ensure accuracy knowing someone can die if we ***** up. The superior that made this 1 patient at a time rule works as the technical director of the blood center. She has book knowledge and no hands on knowledge past when she got her SBB over a year ago. She always has to look up questions she receives or ask one of us. She hasnt worked in a hospital environment in probably 5 years or more. Therefore her attempting to dictate how we should perform bench work when she cant and doesnt is ludicrous. This is the same person who refused to disagree with my supervisor on an incorrect antibody ID I questioned cause she doesnt have the knowledge to recognize that gee the supervisor could be incorrect. She basically agreed with her logic cause she is inept at looking at what's there and analyzing it. How does someone get in this position one might ask-lots of smoozing and you know what kissing and appearing to know what they are doing to those that dont know the difference. Anyone reading this may think I appear bitter and jealous but that is not the case. I pride myself on turning out good results because I care for the patient and I also dont want to lose my license based on turning out something wrong cause my superiors tell me to.
-
Well after all the "isssues" of the past couple of weeks of daring to challenge the powers that be that seem to think they are better than me just cause they are my supervisors the latest is that we are now only supposed to work on one patient at a time. I'm like seriously??? and in what reality??? This is of course coming from someone once again that sits in her office all day and pretends to know blood banking. Supposedly we will "confuse" patients by working on more than one at a time. Of course I have to deal with 6 plus at a time at my other job and the phone and people coming for blood and gee on weekends even another whole department. So yeah I can only handle 1 patient at a time.
-
Well I do pray for the patients. Luckily I work at a blood center with this supervisor and she doesnt know what I advise the clients that send us antibody IDs. In the mentioned things I was questioned on I advised based on what I would do as a tech in a hospital that wanted to immediately transfuse a patient. I do by the way still work per diem at a hospital under a very knowledgable supervisor and she has no problem with my interpretations, which is why I'm pretty much more ****** off than anything cause I'm a good tech and I do care about results I turn out and dont appreciate being questioned about them.
-
The explanation I received today-and she still insists I'm wrong and she's right is that the coworker ruled out C and Fya with the autoabsorption so it had to be a warm auto. She had him perform the autoabsorption on a panel which expired in May, which he had used as a rule out panel and obtained the same sort of results on the top half of the panel-i.e. reacted with C, Fya and K pos cells and was negative with the cells negative for all three. The bottom half of the panel had all negative results. Her interpretation of this was that it was the warm auto reacting weakly cause of the age of the panel. I argued the point that it makes no sense that he shouldnt have obtained reactions on the bottom half of the panel and suggested he forgot to add the plasma. She says its impossible as he did the whole panel at the same time. Obviously she was not sitting there watching him put drops (or not putting drops) of plasma in each tube so he could have erred-it happens. So she has him test 2 cells positive for C and Fya on this aged panel with the auto absorbed cells and they are negative so she claims this ruled them out cause if indeed the alloantibodies were there it would still be positive. I said using that logic why wasnt a K positive cell tested as well since we're all agreeing K is there? The response was eh guess we should have but we didnt. So yeah-I was questioned about recent panels I did which she didnt like my interpretation work up of as a result of this. Unfortunately for me I have 23 years of blood banking experience and I'm at the level that I dont need to reprove everything and dont get whigged out about certain "unexplained" reactions. When a patient is in the process of starting to develop a new antibody or has some other interference from drugs etc you are going to have things that arent always cut and dry. You go with what you know for sure and recommend things like phenotypically compatible/crossmatch compatible blood. She has about 7 years experience and is currently getting her SBB. So she thinks that makes her more knowledgable than me. In some respects I acknowledge that she has new info and I appreciate getting it but I dont appreciate questioning my work. So guess if anyone else reading this novel can explain better than she did how I'm wrong I'm going with I'm right.
-
Thank you for the agreeing that an auto adsorption was NOT the next step. This was reported out as a warm auto and anti-K which is why I was totally uncomfortable reviewing it and saying it was fine as is. So today at work ought to be interesting because my "wrong" reasoning is supposedly going to be discussed with me. My concern was that the patient received Fya and C positive units do to them only calling it anti-K but the units fortunately were negative for all 3. I questioned the warm auto as it clearly had obvious negative cells, which obviously fit a pattern that looks like they are all negative for cells neg for K C and Fya. I'm told that warm auto dont have to react with all the cells. Anyway just have to continue to be a good tech and hopefully wont cause further problems with daring to question a supervisor.
-
unfortunately we do not have any sort of enzyme techniques to use. The person working on this as directed by the supervisor was told to do autoabsorptions as the next step. Yes the auto is positive in gel and negative in PEG but this seems to occur a lot I've noticed with gel as if some other thing is causing the gel to have positive auto controls. The DAT was performed and was negative. My conclusion was the same as yours. I dont have the autoabsorption results but the coworker used 2 cells on the same Immucor panel and then an expired panel. The expired panel showed reactivity and I'm told to ignore it cause it didnt absorb out and needed to be absorbed again. The current panel managed to obtain negative reactions on cells 1 and 2. Coworker also did a peg panel on an older panel and came up with negative cells from 10-16 which leads me to believe the plasma was omitted from the tubes so I'm not buying that the absorption was performed correctly.
-
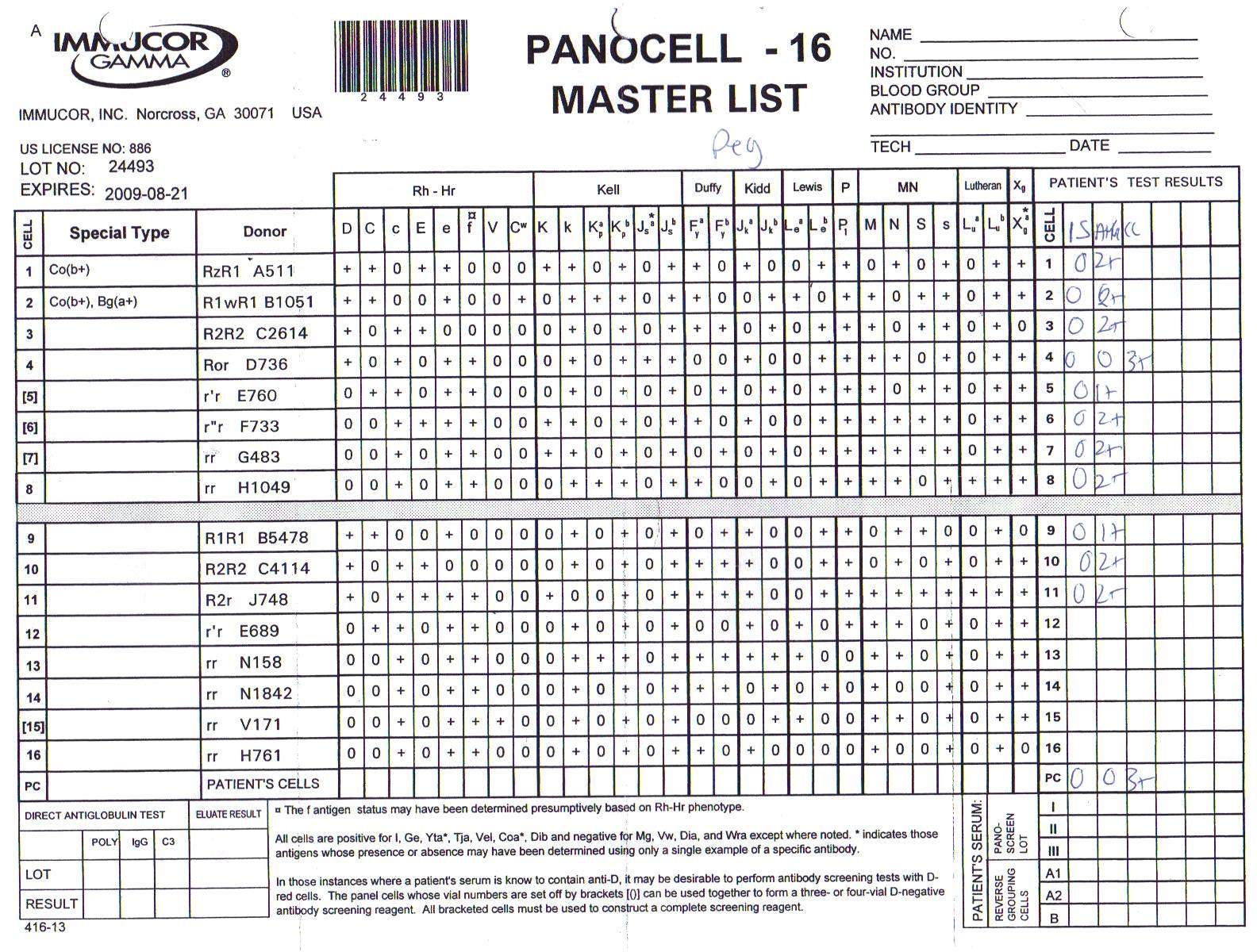
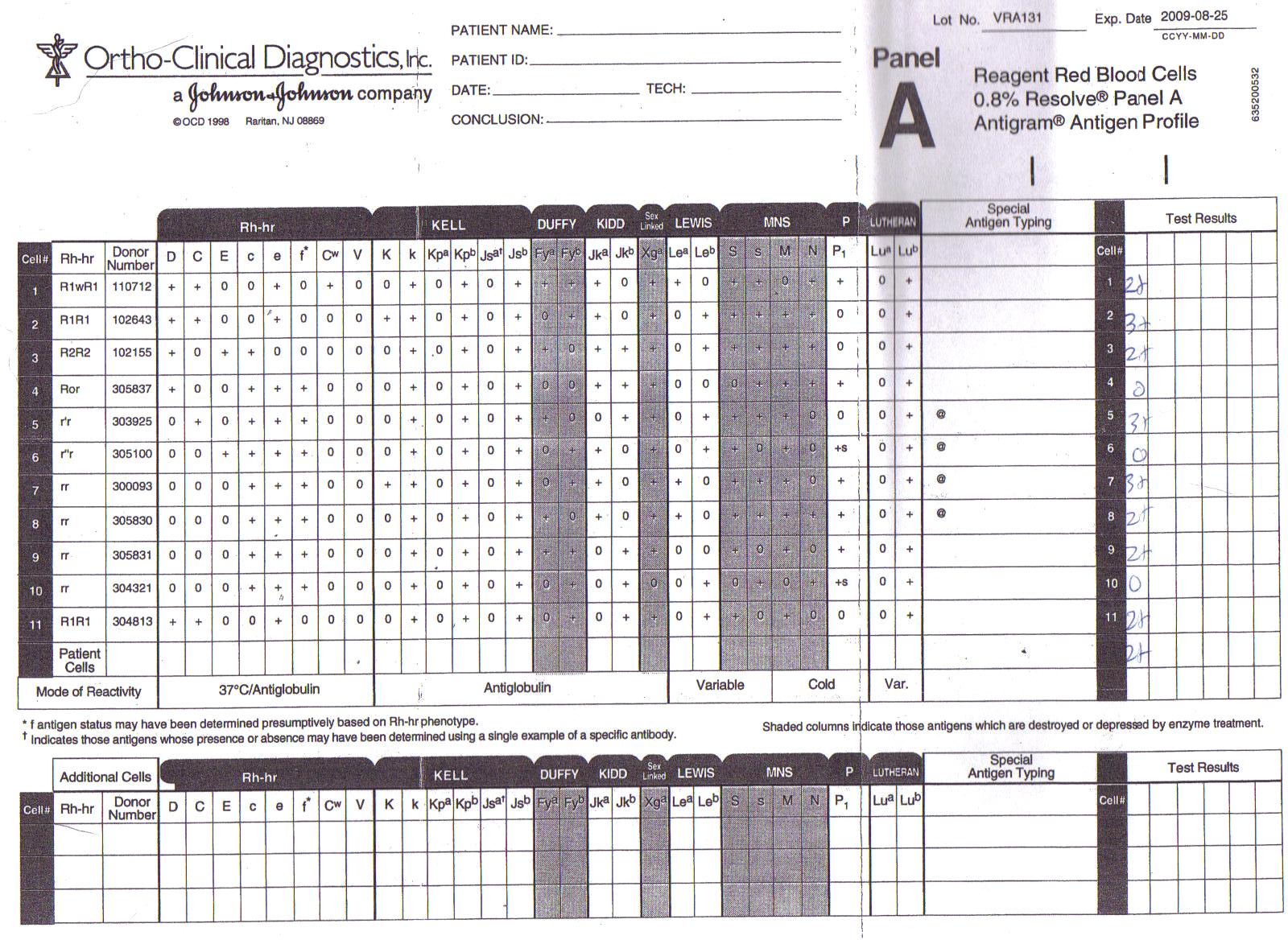
Well here's my attempt at uploading the antigram sheets.

-
I was recently in the position to have to review an antibody ID performed by a coworker. I disagreed with the determination and called our supervisor asking if she had looked at it and was told yes and pretty much dismissed my concern over thinking it was incorrect. So if anyone has these 2 panels and can let me know what their opinion is that would be great. Ortho Gel panel lot VRA131 and Immucor panocell-16 lot 24493 Reactions obtained on gel panel are as follows: Cell # reaction 1 2+ 2 3+ 3 2+ 4 0 5 3+ 6 0 7 3+ 8 2+ 9 2+ 10 0 11 2+ auto 2+ Reactions obtained on Immucor panel with PEG as enhanceent Cell# reaction at AHG-all neg at IS 1 2+ 2 2+ 3 2+ 4 0 5 1+ 6 2+ 7 2+ 8 2+ 9 1+ 10 2+ 11 2+ auto 0 The other thing that assisted me in thinking that I am correct in what I think the antibodies are was based on the patient's phenotype which was also performed along with this panel. Patient is E+e+C-c+ Jka+Jkb+Fya-Fyb+ M+N+S+s+ K- Looking forward to any sort of feedback.