Everything posted by RRay
-
 The MaxQ have thin light blue panels. You can do refrigerated or frozen depending on how you validate. My current facility I validated using all frozen for best temp charts. Previous facilities I used 2 fridge, 3 frozen to get the same time. Might depend on a lot of things. One place was at sea level an super humid, one was 6200 ft altitude and super dry....not sure if that makes the difference. I think MaxQ recommends the fridge and frozen panels b/c the inside is stickered as such but I couldn't validate these that way for whatever reason. All frozen is easier to remember so I'm not mad about it. You can always email the vendor for more info.
The MaxQ have thin light blue panels. You can do refrigerated or frozen depending on how you validate. My current facility I validated using all frozen for best temp charts. Previous facilities I used 2 fridge, 3 frozen to get the same time. Might depend on a lot of things. One place was at sea level an super humid, one was 6200 ft altitude and super dry....not sure if that makes the difference. I think MaxQ recommends the fridge and frozen panels b/c the inside is stickered as such but I couldn't validate these that way for whatever reason. All frozen is easier to remember so I'm not mad about it. You can always email the vendor for more info. -
I have MaxQ MTP coolers. I have validated them for 6 rbc, 6, FFP and up to 2 RT items i the front pouch with an insulated bubble wrap liner. It will validate with 6 warm FFP in the section next to 6 RBCs. The RBCs never even notice. Good for 12 hrs 1-6C for ease of expiration calculation.
-
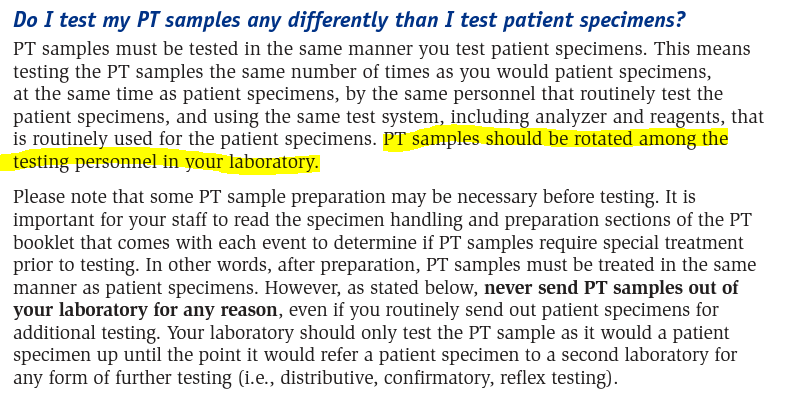
I mean, I guess you could give all 5 samples to one tech if they're the only tech performing the test... but that's doubtful if you're in a university hospital setting.
-
Interesting. I've never read anything on that and couldn't find a reference to it either. I've always divided my samples up so I can also use them for annual competency for the techs. Here's the CLIA/FDA piece: https://www.ecfr.gov/current/title-42/chapter-IV/subchapter-G/part-493/subpart-H And from the CLIA PT booklet it says: https://www.cms.gov/Regulations-and-Guidance/Legislation/CLIA/downloads/cliabrochure8.pdf
-
Yeah. More oversight. CAP's days are numbered at my facility, and I'm pretty sure ACHC doesn't get into blood salvage any deeper than equipment maintenance at best. Luckily we have all of the CAP standards in place, except adding formal reporting to a committee that the TMMD reviews. It was just in documented for OR use. So they tasked me with seeing what other facilities track for QI since there isn't set requirements. I think the metrics we settled on will be fine, but it's always nice to know where we are amongst our peers.
-
For those interested, this is what we have settled on for now unless it comes out that other locations are tracking something else useful: -Post-wash total Hbg >15 (Hct>45) to indicate good wash quality -effluent line clear or not -Also found post-wash heparin concentration of >0.5IU/mL as indicator of poor wash quality, but not sure if this is feasible to test anti-Xa levels... this one is to be continued.
-
Yup! I have all that in place. Our committee just wants to know what quality indicators other locations are using.
-
Thank you for that information, but I'm looking for quality indicators for monitoring/tracking cell saver use. I feel like I have seen a hct of reinfused product being used before. Some sort of data review is part of a CAP requirement: TRM.41550 X 2 Intraoperative/Perioperative Safety and Efficacy The intraoperative and perioperative blood recovery program ensures the safety and efficacy of the recovered blood components. NOTE: Safety and efficacy of recovered products can be measured through various mechanisms, such as through the review of data by institutional committees and monitoring of the intraoperative/perioperative transfusion practices. Evidence of Compliance: * Review of intraoperative/perioperative blood recovery and reinfusion program records AND/OR meeting minutes of institutional meetings
-
We do 7, but this facility did 14 days about 10 yrs ago. I've also worked at a facility that did 30 day samples. As long as you have a clear policy I believe it's up to your discretion but I haven't seen anything greater than 30 days.
-
Would anyone mind sharing the quality indicators used for monitoring cell saver/auto-salvage procedures? This is a CAP standard. Just wanting to see what other folks use for quality tracking.
-
My experience was great also. Only once has Grifols not been able to fill an order (just wash solution) and they called AND emailed to notify that they were only sending 1 box to keep us operational and would then send the rest on a specific date. So nice! With ortho, I don't know what's not coming until it doesn't show up, even with standing orders. Trying to get updates is a losing battle. Every single standing order delivery of cards from ortho arrived late last year, by more than a couple days.
-
I'd recommend using a continuous temp tracker to validate those. If you're not conditioning the panels correctly (thaw for so long after they are frozen, then maintain refrigerated) some of the units can get below 1C. I was always able to validate for 12 hours, easier to calculate the cooler expiration time.
-
Thanks for sharing! I knew there had to be a better way. The snapshot is awful.
-
I've done the full day demo for BioRad and am neutral on it. My old blood center when to it from Ortho gel. My small peeve with that one is that the single row specimen holders for the analyzer tip over so easily! I've used Grifols before and didn't have problems. The lack of enzyme panel is only a slight inconvenience. We ficin treated cells as needed instead (rarely). What issues have you had with Grifols?
-
We currently use the blood admin snapshot and BPAM. I'm curious to if we can include it in the MAR medication admin module. That's the screen nurses use most and blood admin would fit will within it. It's a scrolling timeline that is visually very user friendly. I just don't know if that information is something someone in Lab (me) can see for transfusion information. My problem with the snapshot is that with it being something rarely used for most nursing units, completion audits are awful. I've even found a unit left in "currently transfusing" status for over 48 hrs.
-
Haha! Crickets. After proposals and price lists, the cost was just a smidge more than Ortho with all supplies for a year's worth of testing considered. However, they still do not have FDA approved enzyme panel or special antigen antisera approved for use on the analyzer. However, I was just burned again by another missing Ortho shipment and had to borrow from a neighboring facility.... I'm tempted.
-
We do use BPAM. How does that information populate/record in Epic from BPAM for you? It's the nurses/doctors who are having issue. Right now our BPAM doesn't interface with our LIS Will be rectified in the new year with a new LIS.
-
Does any have this or has had it in the past? Do you find it helpful? My currently facility doesn't really have a formal committee for this and trying to start one. Wondering if these guidelines would be a good place to start as far as topics discussed and goals.
-
I've received a lot of complaints on how transfusions are tracked for the doctors and nursing teams. Those of you on Epic, how are you tracking transfusions as far as start/end and vitals? One request was to add it to the MAR as a medication. This looks like the transfusion tracking utilized in Sunrise Clinical Manager. It's a scrolling timeline with meds listed vertically. I know Epic is super customizable so there has to be a better way than what we are using.
-
I have recently learned that in these forums it's best to include if you want theoretical information (fun to think about) or something that is compliant to any applicable standards and is feasible to implement. Haha! I'd love to get rid of it too, but hard to justify since it's part of manufacturer's inserts and the Vision won't run certain tests without it (unless I suppose you fudge a barcode and include an alternate diluent). It's part of the FDA approved system. I'm assuming the differences between the two diluents are for their specific uses in the system. Dil 2+ is for your red cell dilutions used for ABO/Rh. The Dil 2 is for your DATs and auto controls.. I can't remember which it uses for XM, maybe 2+? The EDTA added makes sense in that regard, but yeah... I think safe testing can be achieved without specialized diluents.
-
! 5.14.1 ABO Group The ABO group shall be determined by testing the red cells with anti-A and anti-B reagents and by testing the serum or plasma for expected antibodies with A1 and B reagent red cells. If a discrepancy is detected and transfusion is necessary before resolution, only group O Red Blood Cells shall be issued.
-
Yes! That is the hardest part. LIS cooperation. It's hard to notify techs to treat a patient differently.
-
Again, the issue at play is that we cannot confirm the patient ABO and the ABO is not clear at initial testing. We understand that weak positive is positive but the issue is having no reaction at all. You cannot confirm type with discrepancy present.
-
If the result is weak, I agree with you.. it is positive. The situation in question is when it is too weak to detect at IS and how we go about resolving it.
-
I don't feel comfortable adding allowance for the 4 drops procedures for a couple reasons: -It's against manufacturer's insert, which clearly lists 2 drops of plasma/serum for backtype (I will not bother with validating the 4 drops!) -I can't find any suggestion for it in the major BB references. @AMcCord Hate to put you on the spot but you referenced this method in older posts (with ISXM provision). Do you know what the reference is/if any?
