Leaderboard
-
-

Neil Blumberg
MembersPoints279Posts -
Malcolm Needs
Supporting Members ☆Points8,992Posts -




Popular Content
Showing content with the highest reputation on 01/24/2025 in all areas
-
Eluate in the Laboratory Diagnosis of Autoimmune Hemolytic Anemia
jtemple and one other reacted to snance for a post in a topic
2 pointsAgree with Dr Blumberg. In an abstract from way back, 1996, Ann Church studied the value of an eluate, reference and abstract below (apologies for quality of print). A Church, S Nance, D Kavitsky. Assessment of Elution Studies in Cases with 37OC Reactive Serum Autoantibodies (SA). Transfusion 1996; 36:161S (Suppl)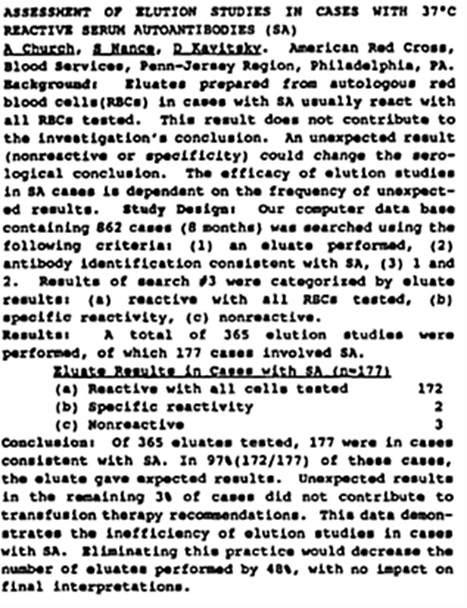 2 points
2 points -
Alarm high/low checks for non-CAP lab.
John C. Staley reacted to RRay for a post in a topic
1 pointPerfect! We are currently on Rees as well. We have a fridge that recommends quarterly alarm checks but that is being replaced soon and that would be the last shred of alarm check suggestion that I see. It is hard to let go of the CAP overlord since JC is so streamlined and often vague. I appreciate your anecdote!1 point -
Alarm high/low checks for non-CAP lab.
John C. Staley reacted to Cliff for a post in a topic
1 pointWe were on the Rees system, a very large facility. They tested on a single probe a year for their high / low check as they said it was the computer that was making the decision to alarm or not. They calibrated each probe. We took all charts off and stopped doing any alarm checks probably 20+ years ago. If a Rees probe or the whole system went down, we had validated thermometers in each fridge, and we'd put a chart on it. We knew we could not rely on the chart, but we would use it in the case of a significant temperature excursion. Maybe the O Pos fridge went a little wonky. We'd review it with the Medical Director and then decide what to do with the products. We never had an issue with AABB or TJC. We were not CAP accredited. When I started as a new tech right out of school, we did not have the Rees system. We had a coop student who would take temps manually once a shift and change all the charts weekly. We did monthly alarm checks - that could take several days. The Rees system had about 100 inputs by the time I left. An automated alarm system is the way to go. We even put an O2 sensor near our LN2 tank.1 point -
Eluate in the Laboratory Diagnosis of Autoimmune Hemolytic Anemia
mpmiola reacted to Neil Blumberg for a post in a topic
1 pointAgree that in “not recently transfused”patients, eluates are of no clinical use unless you like seeing panagglutinins.😜 Negative eluates occur in some drug dependent examples but the clinical information is paramount in such situations in any case.1 point -
Eluate in the Laboratory Diagnosis of Autoimmune Hemolytic Anemia
Neil Blumberg reacted to Malcolm Needs for a post in a topic
1 pointMany, many years ago now, when I was working at the old Westminster Hospital in London as a quite junior member of the Blood Transfusion staff, I spent quite a few hours working on a sample from a patient with a positive DAT, trying to determine the specificity, in order to see whether the antibody was an allo- or an auto-antibody. This included the use of several very rare red cells that I had frozen down and also examining the eluate. After many happy hours, I had got precisely nowhere, and so sent a sample to my former colleges at the International Blood Group Reference Laboratory. I received a somewhat "spicy" report from my heroine Joyce Poole, who explained to me, in words of one syllable, that I had rather been wasting my time, rare cell collection and the laboratory's money as, in almost all cases, the specificity would be found to be an auto-anti-Rh17 or auto-anti-Rh18!!!!! Since then, I have reverted to doing as little as possible on such samples and, when I retired 43 years later, and, as far as I know, none of the patients ever died as a result. There was a close one once, when I was working on a sample on a Saturday on-call in the Red Cell Reference Laboratory at NHSBT-Tooting Centre. I was working on a sample that was overtly a case of wAIHA. After several allo-adsorptions, I was finally able to provide "suitable blood". It was only at the last minute that the computers came back on after an unplanned downtime, and it appeared that the patient was known, from many years previously as having an allo-anti-Vel!!!!!!! As you can imagine, I did several more tests before I released the blood (on Pathologist's orders), as there was absolutely no evidence of an anti-Vel (auto- or allo-) in the present sample - but it did give me a bit of a turn!!!!!!!!!!!! I would recommend a thorough reading of Petz LD, Garratty G. Immune Hemolytic Anemias. 2nd edition, 2004, Churchill-Livingstone. ISBN 978-0-443-08559-8. Other than that and, possibly, looking at the patient's sample at a more molecular level (as noelrbrown suggests above), I really wouldn't do much else, except that I would put a little note with the blood to be transfused to remind the doctors and nurses on the ward to be vigilant with their patient observations. ALL OF THE ABOVE HAVING BEEN SAID, I AM NOT, AND NEVER HAVE BEEN, MEDICALLY QUALIFIED!!!!!!1 point
