jayinsat
Content Type
Store
Profiles
Forums
Blogs
Events
Frequently Asked Questions
Gallery
Downloads
Glossary
Links Directory
Questions
Jobs
Vendors
Everything posted by jayinsat
-
And if you are type O, please consider becoming a regular donor, every 8 weeks. Helpful tip for those who donate regularly, take beef liver capsules to help keep your iron stores up. It is easier on the digestive system than iron supplements. I donate every 8 weeks and hated taking iron because it constipated me or made my stomach upset. Without it, I would have to sit out for a year to replenish my iron stores.
-
@Neil Blumberg, I wish we had you at all of our facilities to educate our medical staff. Sadly, convincing Hematologists and Oncologists (at least here in America) that it is better to postpone platelet transfusions than give ABO incompatible platelets is, more often than not, rejected, especially in light of the fact that many patients are having to wait because of lack of platelet inventory to begin with. What we really need is a push for better transfusion therapy education in medical school. Along with this, continuing education for practitioners needs to become a priority. It is, however, quite difficult to get time with these practitioners. Even when we convince our laboratory medical directors to advocate for these issues, in my experience, clinicians rarely change. All that said to say, in the "trenches," the practice will likely continue to prioritize inventory over safety.
-
Absolutely! It is in our policy in accordance with CAP and AABB standards.
-
We would label the child rh+. The only problem this might cause is if the child returns to our hospital as an adult (we do not treat pediatrics in my facility) and required blood. The initial blood type might seem like a discrepancy since, conceivably, they would initially type rh negative but their historical record would say positive. Of course, we would simply verify this by looking at the previous testing results stored in our LIS.
-
I keep them 10 years (2 years on site) just to be safe. CAP standards are ambiguous and inspectors have been inconsistent. I feel like our LIS has enough proof but I do not want to argue during inspections.

-
Following. I currently just charge for each individual antigen (5).
-
I have used saline filled transfer bags. Normal saline is a similar colloidal mixture as blood products.
-
We do the same as @MAGNUM. Our database is downloaded daily as a background job. It is also downloaded to a network drive so it can be accessed by anyone that has access privilege to the drive from any networked computer.
-
I had this very scenario about a year ago and it turned out mom had an anti-Dia. It was not on any of our in lot screening or panel cells. I did as I suggested and ran a select panel against mother's plasma using expired panel cells and identified the Dia. The eluate on the baby was eluted the Dia also.
-
There could be a number of reasons for this. My first thought is mom could have an antibody against one of the low frequency antigens (Cw, V, Diego, Bg, etc). If you really want to figure it out, you could perform an eluate on the cord blood and a select cell panel on the mom's plasma. You will need to run the cord eluate against that select panel as well. Of course, by select panel, I mean finding panel cells that are positive for the low frequency antigens. That's my thoughts
-
Nancy, I echo everything you said, but I am experiencing the same things in a 400 bed hospital in downtown San Antonio. This is not sustainable and some sort of major intervention needs to happen very soon. After 37 years, I want out of this field.
-
Vacation???? I'd settle for a day off without being called in because we have no staff coverage in the blood bank.
-
Our situation is even worse now than when I originally posted this thread. We are taking candidates with bachelor's degrees in sciences and no lab training. We cannot keep qualified blood bankers. Everyone is burnt out. I am burnt out. The crisis is here.
-
Not only is it quicker to issue 2-4 LTOWB, it is also easier for rapid infusion. The products are supposed to be infused through blood warmers rapidly. This is important to avoid that "lethal triad" of hypothermia, coagulopathy, and acidosis in traumatic bleeds. Whole blood has been shown in studies to be more effective than components in these cases as they can be given quicker and through only one iv access. With 4/4/1, you need at least two lines and possibly more than one rapid infusion pump.
-
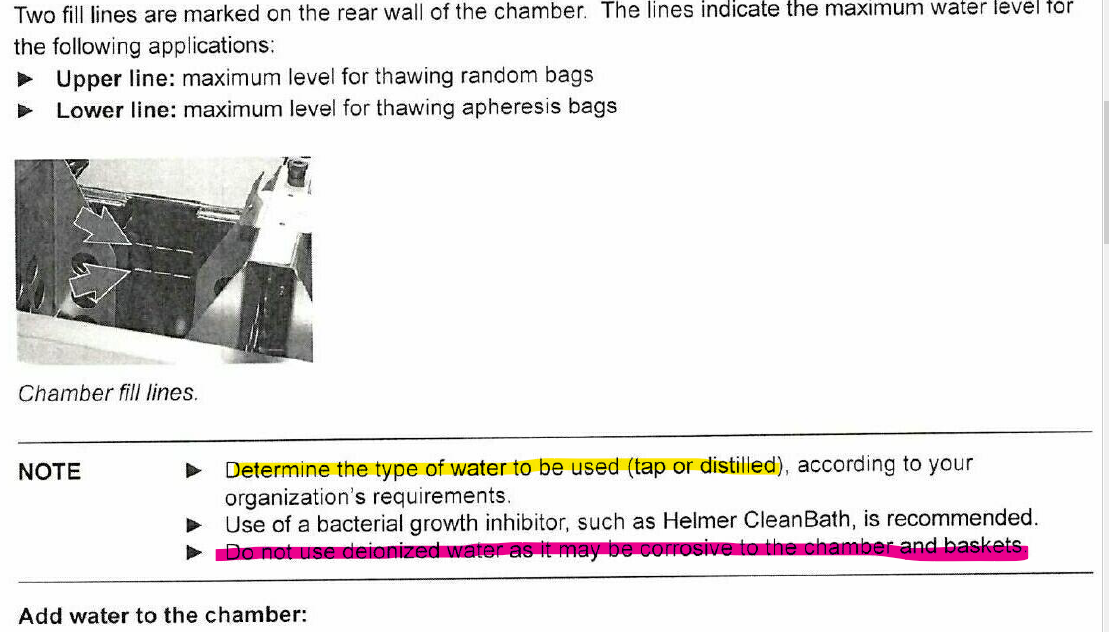
I just replaced mine last month. I used to use deionized water on the old one until I read this (taken directly from the Helmer manual):
-
BloodBankTalk: Clinical Aspects of Transfusion Reactions
jayinsat replied to Cliff's topic in Question of the Day
I just answered this question. My Score PASS -
BloodBankTalk: Correct Blood Bank Nomenclature
jayinsat replied to Cliff's topic in Question of the Day
I just answered this question. My Score FAIL -
BloodBankTalk: QC of multiple reagent racks
jayinsat replied to Cliff's topic in Question of the Day
I just answered this question. My Score FAIL -
BloodBankTalk: Determining eligibility of autologous donors
jayinsat replied to Cliff's topic in Question of the Day
I just answered this question. My Score FAIL -
BloodBankTalk: Blood Transfusion Therapy in Haemoglobinopathies
jayinsat replied to Cliff's topic in Question of the Day
I just answered this question. My Score PASS -
I just answered this question. My Score PASS
-
I just answered this question. My Score PASS
-
BloodBankTalk: Blood Transfusion Therapy in Haemoglobinopathies
jayinsat replied to Cliff's topic in Question of the Day
I just answered this question. My Score PASS -
BloodBankTalk: Can we modify the donor history questionnaire?
jayinsat replied to Cliff's topic in Question of the Day
I just answered this question. My Score PASS