Mabel Adams
Content Type
Store
Profiles
Forums
Blogs
Events
Frequently Asked Questions
Gallery
Downloads
Glossary
Links Directory
Questions
Jobs
Vendors
Everything posted by Mabel Adams
-
Omitting Crossmatch on Emergency Release RBCs
Mabel Adams replied to epfeiffer's topic in Transfusion Services
We do the crossmatches if we have a sample, but there are times as applejw points out when we get no sample, so we document and move on. We supply our helicopters so keep segments from the units which we can use for serological crossmatches if needed. Mostly, we do electronic. -
I am going to tag onto this thread for another question about pre-admit specimens. How do you document that the patient has not been pregnant or transfused? Do they have to sign a form? If so, is that form legal document that must be kept in the records?
-
Has anyone seen a specimen where the red cells were above the plasma after it was centrifuged? The patient was in cath lab and then went for a CABG. I asked our Pharmacy intern to research what meds he got that were more dense than red cells and they said, "the only two agents that are denser than RBCs on the patient's MAR are Calcium chloride (100 mg/mL) and Isovue". The Isovue contrast material is not charted for before the specimen was drawn but later during the CABG. I suspect that is the culprit. His Hct here looks to be about 25% but the redrawn specimen had a Hct of about 45 so I think there was very dense IV fluid in this specimen. Does anyone have similar experience? BTW, this plasma created very junky reactions in gel and interfered with the tube reverse type.

-
Maybe... if I move to the city to be nearer my kids. I was thinking something like this would be good and even helpful.
-
Forty years ago, we occasionally received a mislabeled unit, but I have seen only one since ARC started using more barcodes and related quality practices. That unit was labeled O neg but retyped as O pos. We finally had to return the unit to ARC, and they spiked it to test the contents which were O neg. I think it was early in the Adsol years and we used to get a pedi unit that was CPDA-1 or maybe it had something to do with leukoreduction. When it was collected, the person making segments was in the habit of cutting off the tubing and discarding it but needed to keep it on the CPDA-1 unit for making segments. He quickly realized his error, fished the discarded tubing out of the waste bin and reattached it to the unit, I think with a clamp. Of course, he did not grab the tubing from the correct unit.
-
MTP cut-off policy, or Lethal Dose of Blood Products
Mabel Adams replied to jshepherd's topic in Transfusion Services
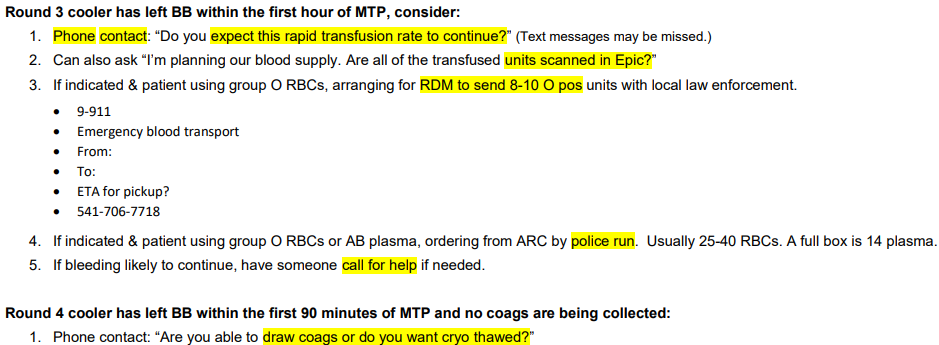
Here are our "nudge" questions. See my other post for our rounds etc.
-
MTP cut-off policy, or Lethal Dose of Blood Products
Mabel Adams replied to jshepherd's topic in Transfusion Services
We created a policy to ask at certain stages whether the MTP is likely to go on at the same rate so we can plan for blood ordering since we are several hours' drive from our supplier. We have this on the back of our MTP log sheet: "Assess Futility? Round 10 cooler has left BB within the first 3 hours of MTP (or inadequate blood supply): • Evidence shows a much-reduced chance of survival if over 40-50 RBCs have been transfused in an MTP. • Pathologist can confer with providers regarding the chance of saving the patient with continued transfusion. • Be prepared to provide pathologist with available blood supply information and expected arrival of more units" Our rounds contain 4 RBC units plus varying yellow stuff. We are starting the conversation at about 40 RBCs, so we have an answer by 50, we hope. We don't have other hospitals nearby that we can borrow more than a few units from. -
As I contemplate retiring in a few years, I would love advice about how to stay mentally stimulated after leaving the field. I have loved medicine since I was 5 years old and suspect that I will miss it after retirement.
-
We accept them back and use them. We put Safe-T-Vue indicators on them, control the refrigerators at some hangars, validate their transport containers and have reviewed the procedures and documentation for storage at the other company's hangar.
-
We are currently TJC, AABB and FDA inspected. They each take a different tack. AABB requires more auditing and data gathering which we sometimes have difficulty doing with current resources. This site has not been CAP in the 14 years I have been here. My previous lab switched to TJC from CAP just after I left there.
-
In the Library on here is a powerpoint that goes through the process. They don't get feedback but it is very step-by-step. I posted it years ago so searching in the files by my name might bring it up. Or it is in the most-downloaded section, it looks like.
-
We have a contract to provide blood to our air ambulances, but they charge the patient if they transfuse it (well, it's wrapped into their total charges for the flight, but we don't charge the patient). If the patient comes to us, we do the XM like we would for our own UNXM units but if the patient is transported elsewhere, we maintain final disposition of the unit in our computer but don't do the XM (yes, we give the patient a fake account in the BB computer using a specific format). It is just easier for us to maintain the record of the unit's final disposition for if there is a market withdrawal etc. We would notify the air transport company to do the patient or next of kin notifications if that were ever needed. It hasn't happened yet so it isn't a big problem.
-
I hope someone can share their policies or criteria for switching O negative patients to getting O positive RBCs due to a blood shortage but NOT when it is uncrossmatched or massive transfusion etc. The usual scenario is that we are on allocation for O neg red cells and have a GI bleed who is usually a male over 50 who needs 1-3 O neg units per day over several days. We don't have other hospitals that we can borrow blood from and we are several hours from our supplier (if they would even release any O neg units beyond our allocation). Have you established a minimum of O neg units that you must maintain for surge capacity if someone with childbearing potential should need several units of O neg? Do you limit how many units of O neg such a patient can take before switching them? Do you try to switch them early if you are going to rather than give them 6 O negs and then have to give them 2 O pos and then they stop bleeding. If you start giving them O pos, when do you switch back to O negs? Yes, we can ask our pathologists but it is they who are asking for some idea of what other places do.
-
Marilyn Moulds is trying to create a blood bank museum. I don't know if it is mostly virtual or not. She can be found on FaceBook these days.
- 1 reply
-
- 1
-

-
We have an opening for a coordinator to support our SafeTraceTx 4.6 system plus several other roles in the transfusion service in our level 2 trauma center. It's a fun and beautiful place to live and a good lab culture to work in. Please message me or use the link below to share about or apply for the position. https://stcharles.wd1.myworkdayjobs.com/External/job/Bend-OR/Coordinator-Blood-Bank-Information-Services--Full-Time--Days-_R1013336
-
I was hoping you would share your experience. Thanks.
-
The Blood Group Antigen Fact Book says HDFN risk of Anti-Kpa is mild to severe. Apparently ACOG says this antibody causes only mild HDFN. Does anyone have any references or know why the book includes "severe"? Our patient has a titer of 32 and we want to manage it like anti-K, but maybe it doesn't affect the red cell precursors like anti-K does.
-
For gel 2+ or less, we ask provider to allow us to send out for molecular typing if patient has childbearing potential. Otherwise, we usually interpret them as D positive but add a note that their type is weak and atypical so they may sometimes be reported as negative and other times (other places) as positive. If they have anti-D or some other reason (anti-C & anti-E?) we will choose to call them D neg.
-
If we get in a directed donor unit with a D00 at the end of the product code, and we want to give it to a different recipient than originally intended, do we relabel it with a V00 product code or can we leave it as D00 and cross it over to regular inventory?
- 1 reply
-
- 1
-
-
What can/cannot be stored with blood products??
Mabel Adams replied to labgirl256's topic in Equipment
I think AABB requires that stored blood products be maintained in a way to reduce errors. The old tradition (maybe there are still rules) of keeping specimens below blood products suggests that specimens spill in the refrigerator. I can't recall every seeing that happen. I've seen a few doozy spills out on the workbenches but not in the refrigerator. -
Update: apparently AABB is changing this standard to an interim standard. Proposed Interim Standard Focusing on Sterile Weld for the 33rd edition of Standards for Blood Banks and Transfusion Services (aabb.org) If the integrity of the weld is complete, and the component is in a container approved by the FDA or Competent Authority for storage, then the original shall have an expiration date/time shall apply, consistent with the storage requirements for the blood or blood component. assigned in accordance with the FDA- or Competent-Authority-approved package insert for the storage container. Standard 5.1.4 applies. Regardless of the integrity of the weld, if no storage time limit is specified in the package insert or the package insert is not available, the component shall have an expiration time of 4 hours after transfer from the original container. Confused yet? I am.
-
I just got information back from Fresenius (now maker of Fenwal transfer packs) that their bags are good for red cells through the unit outdate but that they are not approved at all for platelets. Do you know if Charter Medical says that their bags are approved for platelets? We use their 60 ml syringes and they are listed as okay for platelets so I assume their 150 ml syringes would be but wasn't sure about their bags.
-
One thing we require, before using a pre-warmed technique, is proof that there is room temperature reactivity. You had this with the reverse type but that is often lacking in group O patients. It's not perfect for the anti-Vel etc. but it prevents the habit of doing a pre-warmed technique just to make reactivity disappear. It is a saline method so less sensitive, after all. Using it when you are pretty sure you have a cold can be a reasonable risk to take. Using it when you don't have a cold antibody, means taking an unnecessary risk.
-
Does anyone know a manufacturer of transfer packs that stipulates expiration times? I find nothing online for Fenwal bags and the box doesn't list expirations. Four hours isn't even enough so the product is still in-date at the end of the usually allowed 4 hour infusion time.
-
What is the expiration used for platelets that are divided into a transfer pack/bag using a sterile welder (closed system)? Do you use the original expiration or does the plastic of the transfer bag not allow oxygen transfer like a platelet bag so they have to have a shorter expiration? If the latter, how long of an expiration is permitted?